
Exercise-based ACL & knee ligament injury prevention
In 2018 Arundale, Bizzini, Giordano et al published a CPG reviewing the current injury prevention programs for ACL and knee ligament injuries. The results were extremely positive and state that “there is strong evidence for the benefits of exercise-based knee injury prevention programs, including reduction in risk for all knee injuries and for ACL injuries specifically, with little risk of adverse events and minimal cost” (Arundale, Bizzini, Giordano et al., 2018, p. A7). Prior to researching this blog, I was aware that many injury prevention programs existed, but not clear on what the ideal warm up should include. This blog covers the construct of the most strongly supported programs available as well as two excellent video examples for clinician and patient reference.
As physiotherapists, we often come across patients who are interested in learning more about dynamic warm up exercises that assist in injury prevention. I think we all know there is a lot of information around this topic but it was refreshing to come across a CPG that outlines the ideal components of prevention programs and will now become the basis for my clinical recommendations moving forward.
Summary of recommendations
Clinicians should be recommending the use of exercise-based knee injury prevention programs in athletes for prevention of knee and ACL injuries.
Injury prevention programs should be implemented prior to training sessions or games i.e. as the warm up.
The programs that are most effective require the participant to be active and move and include multiple components of proximal and distal strength, core strength, balance, flexibility, running, plyometrics and agility.
All knee injuries count! Knee-injuries were defined as “any joint pathology including damage to the joint (patellofemoral and/or tibiofemoral), ligaments, meniscus, or patella tendon.” (Arundale, Bizzini, Giordano et al., 2018, p. A3)
This CPG identifies 3 high risk populations and outlines the different programs most suited for each:
Female athletes <18 years of age
PEP, Sportsmetric, Knäkontroll, Harmoknee, Olsen et al, Petersen et al (ACL injuries)
Soccer players, especially women
PEP, Knäkontroll, Harmoknee (knee ligament injuries)
Caraffa et al, Sportsmetric (ACL injuries)
Male and female handball players, particularly 15-17 years of age
Olsen et al, Achenbach et al (knee ligament injuries)
For all programs, the recommendation is that they should involve multiple components, have a session duration >20 minutes, have a weekly training volume >30 minutes, start at pre-season and continue throughout the season with high compliance.
The most supported programs involved multiple components such as
Flexibility - quads, hamstrings, hip adductors, hip flexors, & calf muscles
Strengthening - double-leg squat, single-leg squat, lunges, nordic hamstring exercises
Plyometrics - single leg hopping anterior & posterior, ice skaters, jump to header or catching a ball overhead
Balance & agility
Running - forward & backwards, zigzag running, bounding forward & backwards
Core - prone plank & bridges

Image courtesy of the JOSPT perspective for patients
This CPG actually provides strong evidence to suggest that exercise-based prevention programs reduce the risk of all knee injuries, not just ACL injuries. “The pooled incident rate ratio indicated that exercise-based prevention programs are effective in reducing the incidence of knee injuries (0.73, 95% confidence interval)” (Arundale, Bizzini, Giordano et al., 2018, p. A7). For ACL specifically, the programs are also effective in reducing injury but the pooled ratio rate is lower ranging between 0.38-0.49.
This information within this CPG includes all knee injuries, not just ACL injuries. The evidence and recommendations from this CPG should be used to educate and support coaches, parents, athletes and clinicians to incorporate exercise-based injury prevention programs into their training methods. It seems really important to ensure that this message reaches our young female athletes as they have been identified within each high risk population.
Even though 3 high risk populations were identified, these recommendations should be implemented for all young athletes, particularly 12-25 years of age in high risk sports such as rugby, AFL, netball, soccer, basketball and skiing.
Below are two videos for court and field sports which have been curated and published by the JOSPT and provide a holistic program consistent with the recommendations of this CPG.
Which program to choose?
A key benefit from this CPG is that they provide a decision making tree and specifically list the programs for all knee injuries and ACL injuries. For each article they provide the contents of the program, links to full articles, full reference list and the outline of each article. This allows the reader to broaden their understanding of the programs without having to hunt for the original source.
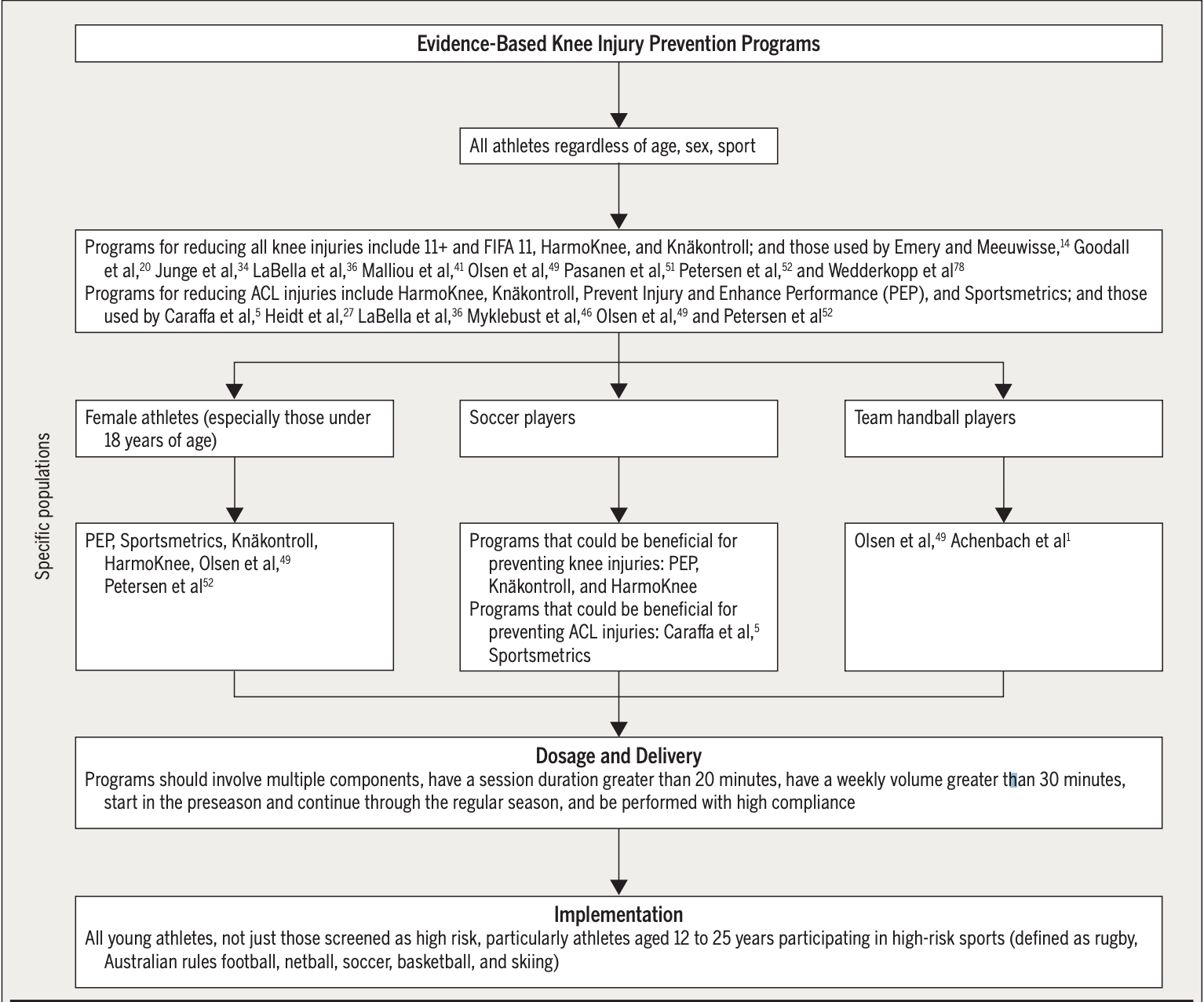
Image from CPG decision making tree https://www.orthopt.org/uploads/content_files/files/Knee%20Injury%20Decision%20Tree%20Figures%281%29.pdf
Fifa 11, Harmoknee, PEP and Sportsmetric are the big fish. Each have their own websites, training programs and resource materials. They also provide sport-specific detail on their website and have video content. But what you might see in the table below is that no single program includes it all and from the CPG, that no single program was recommended as the number 1 program to follow.
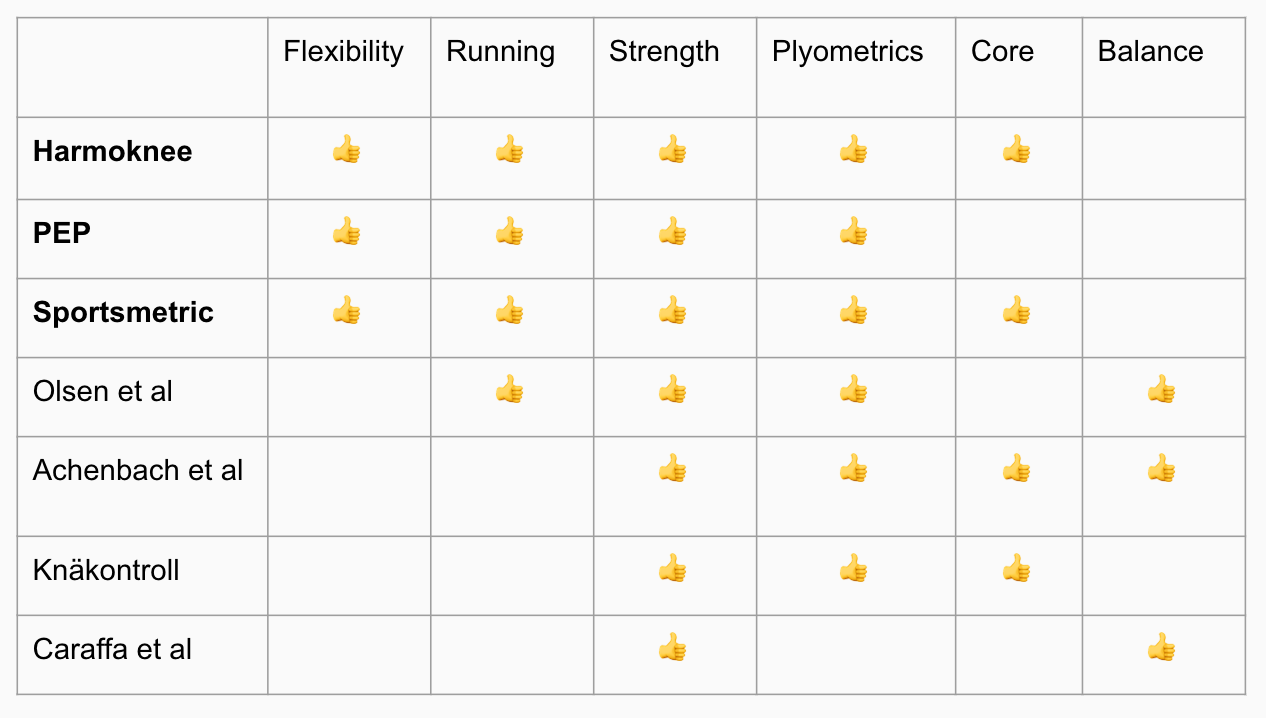
Below is a brief outline of the key programs presented in this CPG and useful links for further information. In the CPG, there is an outline of dosage of each exercise which is not included in this outline.
FiFa 11+
PEP
Flexibility: Calf stretch, quadricep stretch, groin stretch, hamstring stretch, hip flexor stretch
Running: jogging cone to cone, shuttle running, backward running, shuttle run forward and backwards, diagonal run, bounding
Strength: walking lunge, Russian hamstring, single leg calf raise
Plyometrics: lateral hops over cones, forward and backward jumps over cones, single leg hops over cone, vertical jumps over headers, scissor jumps
Sportsmetric
Flexibility: Gastrocnemius and soleus, quad, hamstring, groin, hip flexor, lats, posterior deltoid and pecs.
Running: skipping, side shuffle and running
Strength: back hyperextension, leg press, calf raise, pull over, bench press, Lat dorsi pull down, forearm curl.
Core strength: abdominal curl
Plyometrics: wall jumps, tuck jumps, broad jumps with stick landing, squat jumps, double leg cone jumps side to side, back to front and 180 degrees, bounding in place, vertical jumps bounding for distance, scissor jumps, hop, hop and stick landing, step jump up vertical, mattress jumps, single leg jumps for distance, jump into bounding
Harmoknee
Flexibility: Standing calf stretch, standing quadricep stretch, half-kneeling hamstring stretch, half-kneeling hip flexor stretch, butterfly groin stretch and modified figure-four stretch
Jogging: jogging, backwards jogging on toe, high knee skipping, defensive pressure (zig zig backwards), alternate forward zig zag and backward zig zag running
Strength: lunges, Nordic hamstring strengthening and single leg squat with toe raise
Core stability: sit ups, plank on elbows and bridging
Plyometrics: forward and backward double leg jumps, lateral single leg jumps, forward and backward single leg jumps, double leg jump with or without the ball
In summary, there is no single program to recommend as the best exercise-based injury prevention program and there are many valuable resources available online to help implement such programs into training. Overall, there is strong evidence to suggest these programs are highly effective in injury prevention for all knee injuries. As clinicians, we play an important role in sharing this valuable information with coaches, parents and athletes, to change the way our youth are training and in the hope to reduce injury rates.
To successfully complete these prevention programs requires time and dedication. Realistically there might be as much time spent in warm up as there is in sport-specific training. But the benefits are clear and this message is important to share. This CPG reinforces how important it is for us to teach our young athletes that these warms ups are the foundation for safe training and game play and to reduce the risk of injury, it is not an area we should compromise on. In fact, it might be the most valuable part of attending training and in the long run and keep people in the sport they love for longer.
SS
References/links
Decision making tree for exercise-based injury prevention programs
JOSPT perspective for patients
PEP
Mandelbaum, B. R., Silvers, H. J., Watanabe, D. S., Knarr, J. F., Thomas, S. D., Griffin, L. Y., ... & Garrett Jr, W. (2005). Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up. The American journal of sports medicine, 33(7), 1003-1010.
Sportsmetric
Hewett, T. E., Lindenfeld, T. N., Riccobene, J. V., & Noyes, F. R. (1999). The effect of neuromuscular training on the incidence of knee injury in female athletes. The American journal of sports medicine, 27(6), 699-706.
Harmoknee
Kiani, A., Hellquist, E., Ahlqvist, K., Gedeborg, R., & Byberg, L. (2010). Prevention of soccer-related knee injuries in teenaged girls. Archives of internal medicine, 170(1), 43-49.