
Lateral Epicondylalgia - Pathophysiology & Clinical Assessment
Treatment will always take more thought and more time that you think. Have patience. Nothing complicated was solved quickly.
Introduction
Lateral epicondylalgia (LE or LET), formerly & commonly known as tennis elbow is a condition of lateral elbow pain caused by overuse & repetitive loading of the wrist extensor muscles. “Local tendon pathology may be the result of overuse, underuse, or tensile, compressive, or shear forces, which leave the tendon in a debilitated state” (Coombes, Bisset & Vicenzino., 2008, p.253). It most commonly presents in men and women between the ages of 35-54 (Coombes, Bisset & Vicenzino., 2015).

Image source http://www.247wellness.org/wp-content/uploads/2016/03/elbow-pain.jpg
Lateral epicondylalgia (LE) is a term that means pain over the lateral epicondyle and either this term or lateral epicondyle tendinopathy (LET) are the most clinically and diagnostically accurate terms for this condition. We need to step away from the term lateral epicondylitis as there is no inflammatory component in tendon pathology, and the term tennis elbow as lateral epicondylalgia (LE) impacts a much wider population than tennis players.
There remains to date a lack of consensus on the best treatment approach, which can be frustrating for both the clinician and patient (Coombes, Bisset, Vicenzino., 2015). We have learnt a lot however, from a prominent research group out of Queensland, Australia. Brooke Coombes, Leanne Bisset and Bill Vicenzino have repeatedly published clinical reviews, mater classes and research reviews for the management of LE and this blog aims to discuss the key ideas presented by this group.
There are two points to establish from the beginning:
1. LE is a prevalent, challenging and long lasting problem.
2. Despite this, 83-90% of people recovery with a wait-and-see approach within a year, indicating that the condition is self-limiting for many people (Coombes, Bisset, Vicenzino., 2015, p. 938).
These authors propose that “applying a single intervention, or a one-size-fits all approach, to all presentations of LET is unlikely to be effective in every case” (2015, p. 938). Rather clinicians need to evaluate each individual case by case and provide a tailored rehab program.
This is a blog about lateral epicondylalgia, but also, this is a blog about the elbow joint, because the elbow is often far more complex than we think. It is easy to consider it a simple hinge joint but in fact, it consists of the humeroulnar, radiohumeral and superior radioulnar joints. Many clinicians would agree that elbows are often irritable and tricky to treat. “It is impossible to produce movement in any one of these three joints without producing movement in the other” (Maitland, 1991, p. 171).
Pathophysiology
“The clinical presentation of LE is reasonably straight forward and easy to recognise, which contrasts with a more complex underlying pathophysiology” (Coombes, Bisset, Vicenzino., 2009, p.252).
In 2009, Coombes, Bisset & Vicenzino present a new integrated model for LE seen in the picture below, and in their paper they discuss each facet of this model in depth.

In their 2015 paper, these authors discuss the pathophysiology of LE. It is important to note that this condition is multidimensional. There are tendon cellular and matrix changes, alterations in nociceptive processing and muscle function changes that all feed into LE.
Tendon dysfunction:
From a tendon perspective – research has shown that the cellular changes within the tendon are similar to other tendinopathies. Tendon pathology is now viewed as a continuum from reactive tendinopathy to degenerative tendinopathy. This model has previously been discussed, with a key message being that we no longer view tendon pain as an inflammatory process and tendinitis is no longer a suitable diagnostic term. In regards to LE, these authors discuss the tendon cellular and matrix changes that result in tendon dysfunction and immature healing but also how tendons respond to load and how training promotes healing. “Stress-deprivation adversely affects tendons resulting in increased fibroblasts, decreased longitudinally aligned collagen, decreased tendon stiffness and tensile strength” (Coombes, Bisset & Vicenzino., 2009, p.252-253). What this means is that we must assess each patient to choose an appropriate level to load their tendons in order for them to improve.
Pain system changes:
I’m not sure that there is a single condition that is now considered not to have pain system changes but in the treatment of tendinopathy, there is a large body of research emerging that shows complex central changes occurring in these conditions. Below is one of my favourite pictures from NOI group representing pain system changes is seen below and it really sums up so much about lateral epicondylalgia.

Image source https://pbs.twimg.com/media/Cogx8HkVYAAzch3.jpg
On a more technical level, “substance P and calcitonin gene-related peptide reactive nerve fibres have been located in the proximal ECRB tendon in conjunction with small blood vessels” (Coombes, Bisset, Vicenzino., 2008, p. 253). These guys are potent pain modulators!
In comparison to healthy individuals, those with LE commonly have lowered pain pressure threshold (hyperalgesia) and cold insensitivity (cold hyperalgesia) over the lateral epicondyle. The thermal pain threshold changes don’t affect as many people with LE but as you’ll see in the second part of this blog, it is an important component to consider in assessment for more complex cases.
Motor impairments:
Under this component we are referring to reduced strength and changes in motor control. Coombes, Bisset, Vicenzino (2009) suggest we consider wrist flexion/extension strength, shoulder external rotation strength and other key tendon researches such as Jill Cook focus heavily on supination/pronation motor control. In regards to pathophysiology, remember that LE is a multidimensional condition that involves three main components consisting of the affected muscles, the tendon itself, and the local and central pain processing system.
Clinical anatomy

In the region of the lateral epicondyle of the humerus lies the common extensor origin (CEO) comprising a group of forearm extensor muscles such as extensor carpi ulnaris (ECU), extensor digitorum (ED), extensor digiti minimi (EDM), and extensor carpi radialis brevis (ECRB). Of these muscles it is the deep portion of ECRB thought to be most effected possibly due to it’s proximity to the lateral collateral ligament (LCL) and annular ligament and vulnerability to compression with forearm rotary movements. There is “considerable load sharing between these structures” (Coombes, Bisset & Vicenzino, 2015, p. 939). Using this piece of information, we can see why our assessment should also evaluate the rotary stability of the LCL and movement of the radial head.
Extensor carpi radialis longus (ECRL) is also a forearm extensor and has a proximal attachment to the lateral supracondylar ridge of the humerus. It lies in close proximity to the CEO but many anatomy texts don't list it under the CEO. Extensor indices (EI) also has a close proximity to the CEO, with it’s proximal attachment coming from the posterior aspect of the ulna and interosseous membrane.

These muscles are innervated by the radial nerve directly (C6,C7) or branches such as the deep branch of the radial nerve C7, C8 and the posterior interosseous nerve C7, C8. This is another point of clinical anatomy to consider because it means that we need to clear the low cervical spine and also consider the health/movement of the nerves going through this area of the elbow.
When reviewing the clinical anatomy of the elbow I noticed that the condition LE is often discussed under the elbow chapter but the anatomical representation of the CEO isn’t discussed until you review the wrist. That is, the condition and the anatomy are in two different chapters. It made me wonder what this might imply? Are we focussing too closely on the elbow and overlooking the forearm and wrist functions/postures?
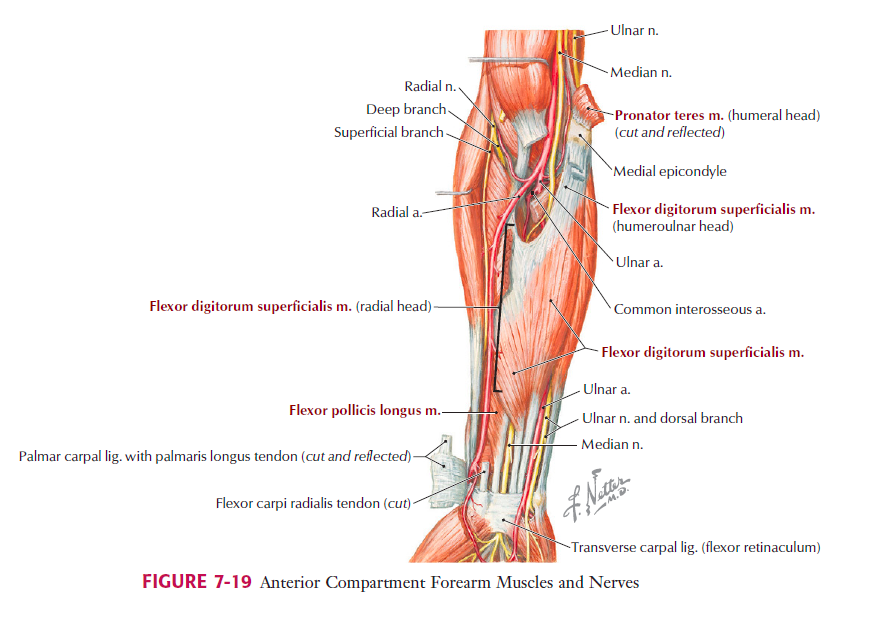
And a final note about the clinical anatomy is the path of the posterior interosseous nerve. As you can see by the image below it lies very close to the CEO.
{kind=link}
{kind=link}
{kind=link}
Image source http://valeriewmsk.weebly.com/uploads/2/3/8/8/23882411/8633463_orig.png
Alicia has previously written about entrapment of the posterior interosseous nerve and I urge you to review this condition if you’re unfamiliar with the key differentiating features between elbow pain associated with LE and that with nerve entrapment.
All of these points combined emphasise that our clinical exam should include:
- Wrist, elbow and forearm range of movement
- Neurodynamic assessment
- Ligamentous stability assessment
- Muscle strength/load tolerance, and
- Palpation.
Clinical examination
The diagnosis of LET is made clinically and our examination should find 3 key features:
- Tenderness on palpation over the CEO at the lateral humeral epicondyle. And not just confirming that the CEO is painful, but that the surrounding tissues are not.
- Pain with resisted extension of the wrist, 2nd or 3rd finger (i.e. CEO muscles).
- Pain with grip (Coombes, Bisset & Vicenzino, 2015, p. 940)
Based on the anatomy and function of this muscle group it is now easy to see why we need these three factors for our diagnosis. But we also learnt that our assessment has to have the three positive factors above but also rule out the five factors below:
- Positive findings on neurodynamics assessment of the radial nerve.
- Altered passive accessory movements of the elbow.
- Limited shoulder range of movement in flexion and external rotation.
- Concomitant neck pain.
- Positive findings instability tests such as the posterolateral rotary draw/pivot shift test and table top relocation test.
From the second list you can see that the exam needs to rule in LE and rule out:
- Cervical radiculopathy.
- Ligamentous instability.
- Intra-articular pathology.
- Posterior interosseous nerve entrapment.
The final area of our assessment is pain severity and functional limitation. For this most papers recommend the patient related tennis elbow evaluation or patient specific functional scale. The PRTEE is a reliable and valid outcome measure for pain and disability. “Scores >54 were considered to represent severe pain and disability, and scores <33 were considered to reflect mild pain and disability” (Coombes, Bisset & Vicenzino., 2015, p. 940). The minimally clinical significant different is 11 points or 37% improvement from baseline.
Some interesting assessment facts from an oldie but goodie (Mack & Burfield, 1997):
- The pivot shift test is done at 45 degrees of flexion which is the most unstable position of the elbow.
- During tennis the triceps and wrist extensors have a huge role in controlling the eccentric moment of the cocking and acceleration phase of the action. Poor eccentric control of pronation is often found in LE patients.
- Lack of extension and supination in a relaxed position is important to assess for, as well as stretch of flexion and pronation. Again coming back to the idea that combined movements of the three elbow articulations are very important to overall function.
- It is important to look specifically at the accessory movement and resting positioning of the radial head. LE patients are often found to have a medially and inferiorly situated head of the radius.
- Ulna sag at the wrist is also found in LE which places the extensor muscles in a different length/tension relationship.
Before we look at treatment for LE I’d like to sidestep for a movement and take a closer look at two key authors. The first is Maitland and his perspective on passive elbow assessment and the second is Shacklock’s teaching on radial nerve assessments.
What does Maitland say about assessment of the elbow joint?
Maitland emphasises in his Peripheral Manipulation text that “examination of passive movements is very important and it is essential for the physiotherapist to know the feel of each joint’s movements. This feel is important in two parts of a movement:
- The first is the friction- and symptom- free quality through it’s full range.
- The second is the feel of the movement at the end of range.” (Maitland, 1991, p. 129).
Yes, I’m quoting a book that was first published in 1970 and republished over 10 years ago because I feel that we are losing touch with the core principles that our professional pioneers were trying to share. Maitland teaches us that we use our passive accessory movements and combined movements to determine if the joint is truly normal. Truly normal means that when active range of movement is painless and full, you still need to full clear the joint before deciding if it is moving normally. “If the term tennis elbow is used accurately, passive movements of the joint will be full range and painless” (Maitland, 1991, p. 189). But often this isn’t the case and patients will have limited shoulder, elbow, forearm and wrist movements, all of which can be contributing factors to tendon overload. During the assessment of passive elbow movement be sure to look at the accessory glides of the three elbow articulations and combined movements such as flexion/adduction, flexion/abduction etc. before confidently saying that the elbow joint is not contributing to lateral elbow pain.
What does Shacklock say about radial nerve assessment?
“The radial nerve neurodynamic test (RNT) applies mechanical forces to the cervical nerve roots and associated spinal nerves and brachial plexus with the scapular depression component and it is likely that the internal rotation component movement applies further stress to the radial nerve as it spirals around the humerus” (Shacklock, 2005, p. 128).
I personally feel that the radial nerve bias of the upper limb neurodynamic assessment techniques is the least discussed and practiced and also a little tricky in terms of handling. The key movements of this test are:
- Scapular depression (taking up the slack, no stretching structures).
- Elbow extension.
- Glenohumeral internal rotation and forearm pronation.
- Wrist and finger flexion.
- Glenohumeral abduction (Shacklock, 2005, p. 129).
The differentiating movements are done for proximal structures by releasing wrist and finger flexion and for distal structures by releasing scapula depression.
Common errors in technique might include: a failure to maintain scapula depression, releasing too much scapula depression during the differentiation process, or excessive pressure on the wrist flexion movement.
The normal response (a covert positive response) includes: pulling in the lateral aspect of the elbow, easing of the sensation with release of scapula depression, and producing a sensation between 0-50 degrees of abduction, which is a large range of movement.
So remember that to qualify an overt positive response you are looking for: reproducing the patient’s symptoms, a significant difference between sides, and a change in symptoms with structural differentiation.
This test is indicated for patients with “posterior shoulder pain, lateral elbow pain, and dorsal forearm pain” (Shacklock, 2005, p. 128). In patients with posterior interosseous nerve (PIN) entrapment, they may report pain over the dorsal aspect of the forearm and exhibit muscle weakness of the finger and thumb extensors without sensory loss (Bisset & Vicenzino, 2015, p. 175). Therefore, weakness of the thumb extensors and pain of the dorsal aspect of the forearm are features associated with PIN entrapment but not LE.
Next we'll take a look at how we design treatment programs for lateral epicondylalgia.
Sian
References:
Amro, A., Diener, I., Bdair, W. O., Isra’M, H., Shalabi, A. I., & Dua’I, I. (2010). The effects of Mulligan mobilisation with movement and taping techniques on pain, grip strength, and function in patients with lateral epicondylitis. Hong Kong Physiotherapy Journal, 28(1), 19-23.
Abbott, J. H., Patla, C. E., & Jensen, R. H. (2001). The initial effects of an elbow mobilization with movement technique on grip strength in subjects with lateral epicondylalgia. Manual therapy, 6(3), 163-169.
Bisset, L. M., & Vicenzino, B. (2015). Physiotherapy management of lateral epicondylalgia. Journal of physiotherapy, 61(4), 174-181.
Coombes, B. K., Bisset, L., & Vicenzino, B. (2015). Management of lateral elbow tendinopathy: one size does not fit all. journal of orthopaedic & sports physical therapy, 45(11), 938-949.
Coombes, B. K., Bisset, L., & Vicenzino, B. (2009). A new integrative model of lateral epicondylalgia. British journal of sports medicine, 43(4), 252-258.
Maitland, G. D. (1977). Peripheral manipulation. Butterworth-Heinemann.
Mulligan, B. R. (2004). Manual Therapy:" nags"," snags"," mwms" Etc. Opt.
Mack J, Burfield H (1997) A new approach in the treatment of tennis elbow. In Proceedings of NZSM, Christchurch “Partners in Action” 77-78
Shacklock, M. (2005). Clinical neurodynamics: a new system of musculoskeletal treatment. Elsevier Health Sciences.