
Pathophysiology & Symptomology of Migraine Headaches

Image courtesy of Google Images
Headaches are a common presenting complaint in the private setting. There are many types of headaches, with some common examples being migraine without aura, migraine with aura, cluster headache, tension-type headache (TTH), chronic paroxysmal headaches, and the one we like to treat, cervicogenic headaches. I'm sure you are all aware that different headache types exist as different clinical entities, but do you know the distinct features of each that aid in our differential diagnosis? Do you know what mechanisms underlie the headache felt in a migraine and what an aura actually is?
Diagnostically, we rely heavily on the subjective assessment to understand symptomatology and the clinical presentation of headaches. To best understand which questions are important to ask, we first need to understand what pathophysiology is likely occurring and how this relates to the patient in front of us.
According to the International Classification of Headaches 3-Beta there are both primary and secondary headaches. Migraine and tension-type headaches (TTH) are considered primary headaches, which are disorders by themselves and not caused by other disorders. Cervicogenic headache (CGH) is a secondary headache, caused by a primary impairment of the cervical musculoskeletal system. The purpose for this blog is to delve deeper into the specifics of primary headaches such as migraine with and without aura and TTH.
Primary versus secondary headaches
PRIMARY HEADACHES:
- Migraine with and without aura
- Tension-type headache
- Trigeminal autonomic cephalalgia, including
- Cluster headache
- Paroxysmal hemicrania
- Short-lasting unilateral neuralgiform headache attack
- Hemicrania continua
- Other primary headaches such as
- Thunderclap headache
- Exercise-induced headache
- Cough-induced headache
- Cold-stimulus headache
- External-pressure headache
SECONDARY HEADACHES:
- Headaches related to trauma/injury such as whiplash
- Headaches related to cervical or cranial vascular disorders such as cerebrovascular accident, intracranial haemorrhage, vertebral artery disorders or vascular malformation
- Headaches related to a non-vascular cranial disorder such as increases cerebrospinal fluid pressure seen in idiopathic intracranial hypertension, non-infectious intracranial disease, neoplasm and epilepsy
- Headaches related substance withdrawal or overdose (caffeine, alcohol, drugs or medication)
- Headaches related to infection such as meningitis, meningoencephalitis, or systemic infection
- Headaches related to disrupted homeostasis such as hypercapnia, hypoxia, hypothyroidism, or hypertension
- Headaches related to disorders of the cranium, eyes, mouth, jaw etc
- Headaches related to psychiatric disorders
The prevalence of primary headaches such as migraine and tension-type headaches (TTH) are much higher than CGH and clinicians need to be equipped with the knowledge to differentially diagnose between these conditions, understand the diagnostic criteria for CGH, and identify red flags for other causes of secondary headache and sinister pathology. Once we understand how to recognise the difference between primary and secondary headaches, we will be more likely to select those best suited for treatment.
What causes a migraine?
"Migraine is a disabling neurovascular disorder characterized by mostly unilateral throbbing head pain and a host of neurological symptoms"(Noseda & Burstein, 2013, p. 1). These neurological symptoms can include a spectrum of disturbances to the perception of light, smell, sound, and effect our cognition, emotions, sensation and motor strength. Migraine really is a challenging condition to define as every individual experiences an array of symptoms. What triggers a migraine differs between individuals and can include a variety of "internal and external triggers such as stress, hormonal fluctuations, sleep disturbances, skipping meals or sensory overload" (Noseda & Burstein., 2013, p.1).
"Migraine headaches are the second most common type of primary headache. An estimated 28 million people in the United States (about 12% of the population) will experience migraine at some point. About 45 % of migraines emerge during childhood and adolescence." (Goodman & Fuller., 2014, p. 1551) The presentation of migraine in children and adolescents differs from that seen in adulthood, with bilateral headache being more common. Migraines are more prominent in females with a 3:1 ratio in prevalence (Buse, et al., 2013) and are often associated with the menstrual cycle (ICHD-3).
"Because of the complexity of this disorder, which is not only limited to its multifactorial origin but also to remarkable premonitory symptomatology, it is thought that migraine headache is a manifestation of a brain state of altered excitability capable of activating the trigeminovascular system in genetically susceptible individuals” (Noseda & Burstein, 2013, p. 1).
To breakdown the neural and vascular mechanism of migraine we can say that a migraine headache depends on:
- The Activation of the trigeminovascular pathway by pain signals that originate in peripheral intracranial nociceptors, and
- Dysfunction of CNS structures involved in the modulation of neuronal excitability and pain (Noseda & Burstein, 2013, p. 7-8).
Pain is the most common complaint. Not every migraine is accompanied by an aura which is why the diagnostic terms migraine without aura and migraine with aura exist (see below). In regards to the headache part of the migraine, activation of the trigeminovascular complex is the key component responsible in the generation and distribution of pain into the head and neck. The cerebral vessels and meninges are innervated by unmyelinated nerve fibres which enter the brainstem via the trigeminal tract and terminate in the trigeminocervical nucleus (TCN). The headache phase of the migraine is through to arise from nociceptive activation of these nerves via chemical, mechanical or electrical stimuli (Noseda & Burstein, 2013). The TCN is the same location of convergence of cervical afferents thought to be responsible for the generation of pain in a cervicogenic headache. Therefore, the headache felt during a migraine has a similar peri-orbital and occipital distribution to a CGH. Even though the distribution of the pain might share similarities the afferent fibres arise from visceral structures (arteries, veins and meninges) causing the headache to have a throbbing quality and be associated with photophobia and phonophobia. In summary, the TCN is currently the main explanation for the pain felt during a migraine, however, the more we learn about the complexity of migraines, the more mechanisms we are discovering.
One of the biggest features of a migraine that is not present in other forms of headache is the aura. Which leads us onto the second main theory of pathophysiology in a migraine; changes in regional cerebral blood flow and the phenomenon known as cortical spreading depression (CSD). Regional cerebral blood flow changes cause cortical spreading depression, which results in the widespread neurological symptoms that come under the description of an aura. CSD is “a mechanism that starts with a small excitatory response that begins to spread through the brain and the causes a suppression of electroencephalographic (EEG) activity that moves through the cortex” (Goodman & Fuller., 2014, p.1554). CSD causes gross disturbances of the brains extracellular environment. There is general consensus that cerebral blood flow changes only occur in migraine with aura, not migraine without aura (ICHD-3) and mostly effects the middle cerebral artery and superficial temporal artery on the side of the migraine (Goodman & Fuller., 2014, p. 1553).
In regards to migraine without aura, it is now clear that it is a neurobiological disorder and research has shown that "glial waves or other cortical phenomena may be involved. The messenger molecules nitric oxide (NO), 5-hydroxytryptamine (5-HT) and calcitonin gene-related peptide (CGRP) are involved."(ICHD-3) These neurotransmitters are found in the meningeal afferent fibres and are released when the TCN is stimulated, resulting in nociception and pain (Goodman & Fuller., 2014, p. 1552). Furthermore, drugs targeting these neurotransmitters have shown to be effective in the treatment of acute attacks.
Aside from the mechanisms discussed in this blog (neurobiological, cortical spreading depression, and trigeminovascular complex) it is also thought that central modulation plays a role in the development in sensitisation and allodynia. "While the disease was previously regarded as primarily vascular, the importance of sensitization of pain pathways, and the possibility that attacks may originate in the central nervous system, have gained increasing attention over the last decades” (ICHD-3).
How do migraines present?
Migraine without aura
Migraines are defined by the ICH as a recurrent headache disorder manifesting in attacks lasting 4-72 hours.
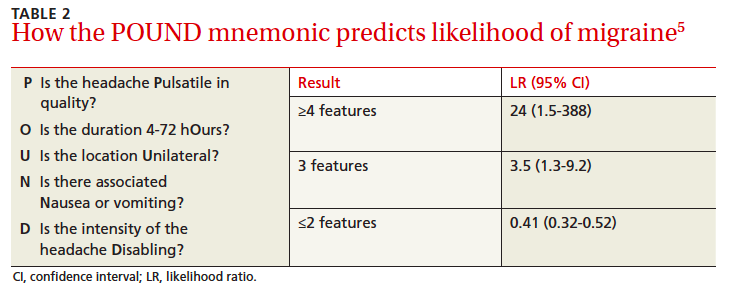
To make the diagnosis of a migraine patients need to have had at least five attacks which last between 4-72 hours and have at least two of the following symptoms: unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity and association with nausea and/or photophobia and photophobia (ICHD-3).
Some other features of a migraine are that they are usually fronto-temporal in position. In children and adolescents migraines vary and are more likely to be bilateral, however if a child presents with a occipital headache (which are rare in children) then this is a red flag calling for diagnostic caution.
(Bissell, Gutmann & Cable., 2013, p. 753)
Migraine with aura
Migraine with aura is defined as a recurrent attack, lasting minutes, of unilateral full-reversible visual, sensory or other central nervous system symptoms that usually develop gradually and are usually followed by headache and associated migraine symptoms (ICHD-3).
For the diagnosis of a migraine with aura patients must experience at least two attacks with the following criteria:
- One or more of the following fully reversible aura symptoms: visual, sensory, speech (aphasia) and/or language, motor (weakness), brainstem, and retinal.
- At least two of the four characteristics:
- At least one aura symptom spreads gradually over ≥5 min, and/or two or more symptoms occur in succession
- Each individual aura symptom lasts 5-60 min
- At least one aura symptom is unilateral
- The aura is accompanied, or followed within 60 min, by headache
What is an aura?
An aura describes neurological symptoms which are related to “transient cortical malfunction and widespread cortical spreading depression” (Noseda & Brunstein, 2013, p.2). While these symptoms usually precede the onset of headache, they can begin during the pain-phase or continue into the headache phase.
Visual aura:
Of the possible auras, visual aura is the most common and occurs in over 90% of patients with migraine attacks (ICDH-3). Visual images changes can include a loss of focus, spots of darkness and zig zag flashing lights (Goodman & Fuller., 2014, p. 1555). The visual aura often begins with a hazy spot close to the centre of vision and the individual may feel their vision is unclear and experience difficulty focussing. Following this, the hazy spot can form into a semicircular shape referred to as a fortification. "This scintillating vision consists of luminous bright, flickering colours of the spectrum, much like a prism catching light. It can be combined with a scotoma, or an area of vision that appears to be obstructed, or missing. The visual image fades and the headache begins” (Goodman & Fuller., 2014, p.1555).

Image courtesy of Google images
Visual Aura Rating Scale
The VARS score is the weighted sum of the presence of five visual symptom characteristics:
- Duration 5-60 min (3 points),
- Develops gradually > or = 5 min (2 points),
- Scotoma (2 points),
- Zig-zag lines (2 points), and
- Unilateral (1 point).
The maximum score is 10 points. A VARS score of 5 or more diagnosed migraine with aura with a sensitivity of 91-96% and a specificity of 96-98% (Eriksen, Thomsen & Olesen, 2005).


Sensory aura
Sensory aura most commonly involves pins and needles “moving slowing from the point of origin and affecting a greater or smaller part of one side of the body, face and/or tongue. Numbness may occur in its wake, but numbness may also be the only symptom” (ICHD-3).
Prodrome symptoms
"Premonitory symptoms may begin hours or a day or two before the other symptoms of a migraine attack (with or without aura). They include various combinations of fatigue, difficulty in concentrating, neck stiffness, sensitivity to light and/or sound, nausea, blurred vision, yawning and pallor. The terms “prodrome” and “warning symptoms” are best avoided, because they are often mistakenly used to include aura.” (ICHD-3).
Migraine with brainstem aura
You may notice that in the list of possible aura symptoms above that brainstem aura is listed. These migraines doesn’t have motor weakness but show at least two of the following brainstem symptoms: dysarthria, vertigo, tinnitus, hypacusis, diplopia, ataxia, and decreased level of consciousness. (ICHD-3) As you can see this is a different subset of clinical symptoms that your patient may report and are associated with disruption to the vascular blood flow from the basilar artery to the brainstem. Many of these patients have the typical aura symptoms, no motor symptoms, and brainstem features.
Retinal migraine
Retinal migraine is a migraine with “repeated attacks of monocular visual disturbance, including scintillations, scotomata or blindness” (ICHD-3).
What is a tension-type headache?
A tension-type headache (TTH) is another highly prevalent form of primary headache. The exact cause of TTH remains unclear but peripheral pain mechanisms are thought to play a strong role. TTH can be differentiated from migraine with the following clinical symptoms (ICHD-3):
- At least 10 episodes of headache occurring on <1 day per month on average (<12 days per year).
- Lasting from 30 min to 7 days.
- At least two of the following four characteristics:
- Bilateral location
- Pressing or tightening (non-pulsating) quality
- Mild or moderate intensity
- Not aggravated by routine physical activity such as walking or climbing stairs
- Both of the following: no nausea or vomiting, and no more than one of photophobia or phonophobia
Red flags relating to headaches
"Headache can be a symptom of neurological impairment, hormonal imbalance, neoplasm, side effect of medication, or other serious conditions. Headache may be the only symptom of hypertension, cerebral venous thrombosis, or impending stroke. Sudden, severe headache is a classic symptom of temporal vasculitis (arteritis), a condition that can lead to blindness if not recognized and treated promptly." (Goodman & Snyder., 2013, p. 553)
The follow list of symptoms are specific to red flags associated with headache that warrant referral to a medical practitioner (Goodman & Snyder., 2013, p. 555):

{kind=link}
{kind=link}
Image courtesy of Google images
{kind=link}
- Headache that wakes the individual up or is present upon waking (e.g hypertension, tumour).
- Headache accompanied by documented elevated blood pressure changes.
- Insidious or new onset of headache (less that 6 months).
- New onset headache with associated neurologic signs and symptoms (confusion, dizziness, gait disturbance, motor disturbance, fatigue, irritability or mood changes).
- New onset of headache accompanied by constitutional symptoms (e.g fever, chills, sweats) or a stiff neck (infection, arteritis).
- Episodes of "blacking out" during headache (seizures, hemorrhage, tumor).
- Sudden severe headache accompanied by flu-like symptoms, aching muscles, jaw pain when eating and visual disturbances (temporal arteritis).
- No previous personal or family history of migraine headaches.
Tips for patient interviewing
Here are some helpful differentiating questions you can ask your patients about their headaches with the primary goal of being able to distinguish between headache types based on symptomatology. With headaches I find it very helpful to map out the symptoms on a body chart as it gives a great visual representation of how patients describe their symptoms.
- Where does you pain begin and how long does it last (CGH will begin in the neck and Migraine in the head)?
- How would you describe your headache?
- Pulsating, throbbing, severity, etc.
- Are there autonomic symptoms and do they dominate the headache and when do they begin (Nausea, vomiting, dizziness, dysarthria, dysphagia, double vision, photophobia and phonophobia)?
- Is your headache unilateral or bilateral? (CGH is usually unilateral and side-locked. Migraine is unilateral but can switch between sides.)
- Does you headache change with drugs such as ergotamine or sumatriptan (medication that alters cranial blood flow)?
- Are there any aggravating movements/positions that bring on your headache or aggravate your headache while it is present?
Physical therapists are best suited to manage clients with cervicogenic headaches with treatment directed to the primary impairments of the cervical spine (painful joint segment, loss of range of motion, muscular impairments). In order to accurately select patients suitable for treatment and differentiate CGH from migraine, it is very important to adjust our subjective examination to specifically identify the symptomatology of each headache type. The aim of this blog was to break down the neuro-pathophysiology relating to migraine with and without aura to better help you understand how these headache types occur and therefore why they will not respond to physical therapy treatment in the same manner as cervicogenic headaches.
Sian
References
Boisselle, C., Guthmann, R. A., & Cable, K. (2013). What clinical clues differentiate migraine from sinus headaches?.
Eriksen, M. K., Thomsen, L. L., & Olesen, J. (2005). The visual aura rating scale (VARS) for migraine aura diagnosis. Cephalalgia, 25(10), 801-810.
Goodman, C. C., & Snyder, T. K. (2013). Differential diagnosis for physical therapists. Elsevier Health Sciences.
IHS Classification ICHD-3 Beta https://www.ichd-3.org/ accessed October 31, 2016.
Noseda, R., & Burstein, R. (2013). Migraine pathophysiology: anatomy of the trigeminovascular pathway and associated neurological symptoms, cortical spreading depression, sensitization, and modulation of pain. PAIN®, 154, S44-S53. Chicago