
Can we pick the clinical signs of excessive sleepiness & sleep disorders?
This blog aims to review what I learnt about the clinical assessment of sleep disorders and hopefully raise some questions about how well we address poor sleep hygiene and identify sleep disorders as a possible barrier to recovery. There is a strong bidirectional relationship between sleep disorders and serious medical conditions such as cardiovascular disease, depression, hypertension and cerebrovascular disease (Bloom, et al., 2009). To better understand our patient's health we need to assess all facets relating to their physical health, mental health and general wellbeing, which includes understanding the quality and quantity of sleep (Pilcher, Ginter & Sadowsky., 1997). The purpose of this blog is to broaden your knowledge about common sleep disorders and to understand what questions can be incorporated into the subjective examination to improve patient assessment and identification of sleep disorders.
Clinical examination
Subjective examination
The history is the most important part of assessing a patient with a sleep disorder as it provides the most accurate description of symptoms and guides further assessment (Bloom, et al., 2009). Having a family member in the room is very helpful because they are the ones who witness first hand the sleep behaviours and their observations are often different to that of the patient.
Commonly people with sleep disorders may complain of:
- Not sleeping well at night,
- Being too sleepy during the day,
- Snoring loudly,
- Kicking legs at night,
- Having excessive muscle and mental fatigue,
- Feelings of depression.
Questions which are specific to sleep that can be included in the subjective assessment (Bloom, et al., 2009):
- Is your sleep refreshing?
- How much sleep do you need to feel refreshed?
- What time do you normally go to sleep and wake up each day?
- How much trouble do you have falling asleep?
- How often do you wake at night to go to the bathroom?
- Is it difficult to fall back asleep?
- Is there a family history of sleep disorders?
- What does your bed partner say about your sleeping behaviours?
- Do you snore, gasp for air, have episodes of restlessness, or experience nightmares?
- Does your partner ever say you kick, thrash, punch, scream or walk during the night?
- Do you feel sleepy or tired during the day?
- Do you fall asleep unexpectedly during the day?
- How many naps do you take during the day?
- How much exercise do you perform during the day?
- How much caffeine or alcohol do you consume each day?
- How is your general health (cardiovascular, respiratory, gastrointestinal etc)?
- How is your mental health? Do you suffer from anxiety, stress or depression?
- What is your social history?
- What medication do you take? Do you suffer from any side effects relating to this medication?
Epworth Sleepiness Scale
A good alternative or addition to questioning during the subjective history is to get your patient to fill out an outcome measure. The Epworth Sleepiness scale is a validated and widely used outcome measure for the assessment of daytime sleepiness. Excessive daytime sleepiness is the biggest indicator of whether or not our sleep is restorative and functional. It involves 8 questions which are answered on a four point scale 0-3.
How likely are you to dose off or fall asleep in the following situations in contrast to just feeling tired?
0 = never, 1 = slight chance, 2 = moderate chance, 3 = high chance of sleeping.
- Sitting and reading
- Watching t.v
- Sitting, inactive in a public place (theatre or meeting)
- As a passenger in a car for an hour without a break
- Lying down to rest in the afternoon
- Sitting and talking to someone
- Sitting quietly after lunch without alcohol
- In a car, while stopped for a few minutes in traffic.
What is your score out of 24?
Excessive sleepiness is >10/24 but there is no strict cut off for this and there is also a poor correlation with objective measures of defining sleep disorders. Despite this, it is still commonly used as a questionnaire as it provides a reliable way to measure subjective symptoms and strengthens the subjective examination.
The ESC pdf can be accessed here.
Physical examination
Sleep tests are used to define the sleep disorder and determine severity. A physical examination of the upper airways and throat also provides information about anatomical contributors to sleep disorders and predisposing factors. Objective measures of sleep include polysomnography and sleep latency tests.
A polysomnography will include the following:
- Diagnosis and assessment of breathing patterns and will distinguish between abnormal sleep behaviours.
- EEG electroencephalogram
- EOG electrooculogram
- EMG electromyogram
- ECG electrocardiogram
- Snoring
- Nasal and oral airflow
- Chest and abdominal movement
- Pulse oximetry.
Some of the suspicious sleep activity would include > 5 apnoeas or hypopneas per hour of sleep, O2 saturation levels dropping below 90%, and > 15 periods of limb movements per hour of sleep. These factors would direct doctors towards the diagnosis of obstructive sleep apnoea, parasomnias and sleep related movement disorders.
Sleep latency tests (time taken to fall asleep) and hypnograms provide temporal summation of sleep showing us how much time is spent in each state of sleep including the duration, latency (time taken to reach each stage), frequency of episodes. All of these are important markers to evalutate the quality of sleep both clinically and experimentally. For example, if someone goes from wake to REM sleep without passing through NREM sleep, it is a sleep disorder called narcolepsy. Another example is if there is a long latency between wake and NREM sleep, it is diagnosed as insomnia.
Do you get enough sleep & Is it good quality sleep?
The image below gives an overview of how much sleep we really need at different stages of our lives (National sleep foundation). Getting enough has been strongly associated with increased satisfaction with life, improved mood, reduced depression and anxiety, and a more positive sense of well-being (Pilcher, Ginter & Sadowsky., 1997). There is a high possibility that most people reading this blog don't get enough sleep.
For adults the average hours of sleep required each night is 8 hours.
An American study conducted out of the Seattle Children's Research Institute, Seattle, Washington, investigated and compared data between adolescents with chronic pain and healthy controls (Law & Dufton, 2012). The average adolescent was 15 years old, 73% of the participants were female, 82% were caucasian, within the pain group 27% reported neck pain, 20% abdominal pain, 43 % musculoskeletal and the remaining uncategorised. The authors thought that adolescents with pain would have both nocturnal and daytime sleep abnormalities. Their results didn't confirm their hypothesis. What the data showed is that all adolescents slept on average 7 hours a night, meaning all participants were sleep deprived regardless of if they were in pain or not. Those with pain had a great tendency to nap for over 30 minutes during the day with 2/3 of the pain group napping more than once each day. The authors suspect that this greater tendency for daytime napping may be related to medication use, which fell into three groups: antidepressants, anticonvulsants and opiod medications. Certainly the results of this study are consistent with what I learnt during the sleep course, that all CNS medication impacts sleep.
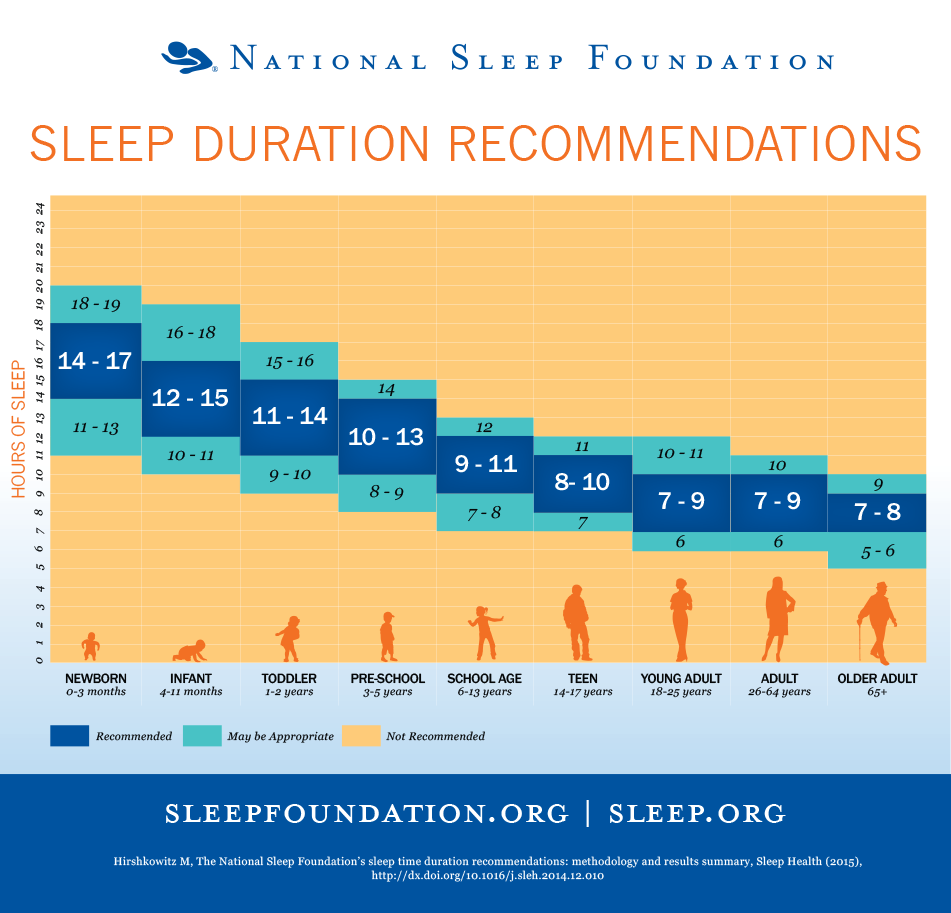
National Sleep Foundation http://sleepfoundation.org/sites/default/files/STREPchanges_1.png
Healthy sleeping habits
The National Sleep Foundation recommends the following tips for establishing Healthy sleeping habits:
- Stick to a schedule the best you can.
- Practice a relaxing bedtime ritual - this includes not working in the bedroom.
- Don't go to bed to sleep unless you're tired.
- If you're having trouble falling asleep then avoid daytime napping.
- Exercise daily "Any exercise is better than no activity".
- Make the bedroom as comfortable as possible. The room should be cool - we sleep better when we are cooler. The bed must be comfortable and minimise the noise and light.
- You spend 1/3 of your life in bed sleeping so invest in a comfortable pillow and mattress.
- Bright light drives the circadian rhythm. Avoid it before bed and use it in the morning to wake up.
- Heavy meals, alcohol and caffeine all disrupt our natural sleeping cycle therefore try minimise exposure to these right before bedtime.
- Use the bedroom for sleep and sex so that there is a strong association between the bed and sleeping. Try to avoid using the bed for working as it weakens this association.
Classification of sleep disorders
- Insomnia
- Insomnia is not just trouble falling asleep. It is actually a problem initiating sleep, maintaining sleep, waking up too early and an inability to get restorative sleep despite an adequate opportunity and environment to do so. Insomnia is either primary or comorbid and effects 10-20% of the population (Bloom, et al., 2009).
- Obstructive sleep apnoea
- Central disorders of hypersomnolence
- Narcolepsy type 1
- Narcolepsy type 2
- Idiopathic hypersomnia
- Kleine-levin syndrome
- Circadian rhythm disorders (jet lag and shift work)
- Parasomnias (abnormal behaviours)
- Sleep walking
- Sleep terrors
- Sleep related eating disorders – when you eat food during your sleep that you’re trying not to eat while awake
- REM sleep behaviour disorder – acting out your dreams, which is often violent
- Sleep enuresis (bed wetting)
- Sleep related movement disorders
- Restless leg syndrome
- Periodic limb movement disorders
- Sleep related bruxism
- Sleep related rhythmic movement disorders.
I’m just going to expand on one of these – Obstructive Sleep Apnoea (OSA) - because I gained the impression during the course that this is sleep disorder affects the most people and that it is poorly diagnosed and recognised. If more people were aware of the symptoms then better diagnosis and treatment could occur. In the older population OSA has can affect 70% of men and 56% of women (Bloom, et al., 2009, p. 769).
OSA is a condition driven by the brain which only occurs during sleep. It is categorised by >10 seconds of not breathing and >5 episodes of apneoas during a sleep hour. That’s about 50 seconds on not breathing while sleeping resulting in oxygen deprivation to the brain. How long can you hold your breath for? OSA is caused by anatomical narrowing of the airways, excessing collapsibility of the throat and abnormal neural control of the muscles lining the throat.
The typical individual presenting with OSA will have the following traits; excessive daytime sleepiness, male gender, overweight, loud snoring at night, middle ages and older, lack of energy, insomnia, and reflux.
There are many serious adverse effects of OSA relating to oxygen deprivation in the brain. These include increased risk of developing:

- Hypertension
- Mortality, Stroke, & TIA
- Myocardial infarction, Cardiac arrhythmia, & Heart failure
- Metabolic syndrome & Diabetes
- Depression & Dementia
- Asthma
- Reflux
- ADHA
- Erectile dysfunction
The most commonly recommended and used treatment of OSA is CPAP (continuous positive airway pressure). One of the biggest barriers to treatment is poor knowledge of the general public about the signs and symptoms and treatment options. Other treatment modalities include 6-8 weeks of intense cognitive behavioural therapy (CBT) but many psychologists have limited training in CBT for sleep disorders which prevents access to treatment.
Summary
The aim of this blog was to outline common sleep disorders and demonstrate which questions can be used during the subjective examination to identify abnormal sleep. I was surprised by how easy these questions are to remember and ask to incorporate into my usual assessment. I encourage all of you to practice using them in your patient assessment just the same way we question about red flags. Remember your patient is the most useful source of information to help you understand their problem. Perhaps we need to consider how much poor sleep can be impacting their pain? The next blog aims to explore the research linking sleep disorders and sleep deprivation to chronic pain and pain sensitivity.
Sian
Further resources for assessment of sleep disorders
American Association of Sleep Apnoea
National Sleep Foundation e-book on sleep disorders
Insomnia sleep test by Online-Therapy.com
International Classification of Sleep Disorders
For further information about the assessment and management of sleep disorders in the ambulatory setting I would recommend Bloom et al (2009) which reviews specific questioning of each sleep disorder and reviews what medications may be impacting that condition. This review covers each of the conditions listed above.
References
Bloom, H. G., Ahmed, I., Alessi, C. A., Ancoli‐Israel, S., Buysse, D. J., Kryger, M. H., ... & Zee, P. C. (2009). Evidence‐based recommendations for the assessment and management of sleep disorders in older persons. Journal of the American Geriatrics Society, 57(5), 761-789.
Law, E. F., Dufton, L., & Palermo, T. M. (2012). Daytime and nighttime sleep patterns in adolescents with and without chronic pain. Health Psychology,31(6), 830.
Pilcher, J. J., Ginter, D. R., & Sadowsky, B. (1997). Sleep quality versus sleep quantity: relationships between sleep and measures of health, well-being and sleepiness in college students. Journal of psychosomatic research, 42(6), 583-596.