
Hip: Ligamentum Teres
Last month Sian wrote a reflection from the lecture she attended presented by Joanne Kemp on FAI, a diagnosis that has gained much traction over the past decade. Ligamentum teres (LT) pathology is also a hot topic in the sporting physiotherapy world with many people speculating unnecessary surgery is being performed. I wanted to know if ligamentum teres really causes pain or is it a vestigial structure? I decided to provide an update on current literature regarding the function, pathology and management of ligamentum teres, to attempt to answer these questions.
Anatomy
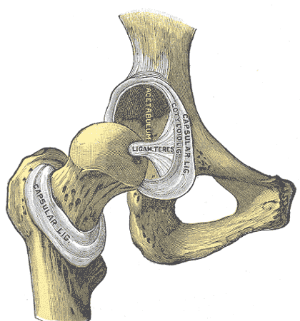
The ligamentum teres is a triangular band made of 1-3 bands or bundles attaching from the acetabulum to the fovea (Bardakos & Villar, 2009). It's been described as similar to the anterior cruciate ligament (ACL) as both are intra-articular with a bundled appearance and similar ultimate load to failure. However, ligamentum teres does not have fibrocartilaginous attachments, it has more nociceptors than the ACL, there's no experimental data on the bundles, and in general, the anatomy is poorly researched (Bardakos & Villar, 2009).
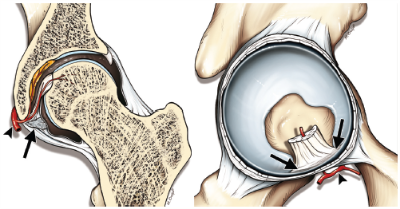
Anatomy of Ligamentum Teres. Bardakos & Villar (2009)
Functions of Ligamentum Teres
The following have all been proposed as functions of the ligamentum teres so we will look at these further.
Blood Supply
This ligament was originally thought to provide blood supply to the femoral head, however one third of adults don't have arterial sufficiency. So possibly ligamentum teres only supplies blood in an immature skeleton (Cerezal et al., 2010).
Synovial Fluid
In 1997, it was proposed the ligamentum teres distributes synovial fluid using a windscreen wiper effect, however this is a theory only with no other evidence to support it. In particular, recent studies doubt this theory (Bardakos & Villar, 2009).
Proprioception
Various studies have found somatosensory afferent Type 4a fibres in the ligamentum teres which are associated with blood vessels and vasomotor function. These are classified as nociceptors but also have a role in proprioception and fine motor coordination, so some proprioceptive role is probable (Haversath, 2013).
Nociception
Here, my question of "can the ligamentum teres cause pain?" is answered. Pain-associated nerve fibres are in the highest concentration in the mid-third of ligamentum teres. However Botser and colleagues (2011) found no correlation between patient's hip VAS scores and the presence or the size of a ligamentum teres tear. Also, other structures in the hip (capsule, chondral surface, labrum) have a larger number of pain-fibres (Haversath et al., 2013). So although the ligamentum teres can produce pain, it appears to be overshadowed by other structures (Chang et al, 2014).
Stability
Ligamentum teres was previously thought of as a straight band, being tightest in:
- flexion/adduction/external rotation - pigeon pose (Bardakos & Villar, 2009)
More recent studies show it's tightest on
- flexion/external rotation - feet turned out squat
- extension/internal rotation - cross leg behind (Haversath et al., 2013; Martin, Palmer & Martin, 2012)
However, current thinking follows the ligamentum teres provides a sling-like structure preventing inferior subluxation especially on squatting movements (Kivlan et al., 2013; Martin et al., 2013). A study by Kivlan and colleagues (2013) showed 100% of complete ligamentum teres tears with existing bony abnormalities (femeroacetabular instability, dysplasia) complained of instability on squatting, which correlates with both these theories.
Mechanism of Injury
Ligamentous injury occurs with uncontrolled movement when the ligament is on maximal tension. Mechanisms include a fall on a knee with hip flexed (flexion/adduction stress), a sudden twisting mechanism (external rotation), hyperabduction with/without avulsion (such as ballet, gymnastics) and surgical dislocation (FAI surgery, total hip replacement) (Botser et al., 2011; Cerezal et al., 2010). However Botser (2011) described only 9 of 28 full thickness tears being an acute onset with four of these being traumatic. It appears tears are more likely degenerative, caused by a wearing of the ligament rather than an acute injury.
Acute injury often occurs in high impact sports (such as hockey and football) and activities requiring extreme range of motion (such as gymnastics and dancing) (Cerezal et al., 2010). Haviv (2011) found all isolated ligamentum teres tears were in dancers, gymnasts or those performing calisthenics, so possibly the hyperabduction and sudden twisting mechanisms are more common than falling.

Signs & Symptoms
- Signs and symptoms are very hard to differentiate, allegedly it causes groin pain related to activity, sometimes radiating to medial thigh.
- There could be painful clicking, locking, giving way (exactly same symptoms as labral tear description by Philippon (2012)).
- The literature is split on hip ROM, with half saying it’s reduced (Bardakos & Villar, 2009; Byrd & Jones, 2004) and half saying increased ROM (Botser et al., 2011; Cerezal et al., 2010), with the more recent literature suggesting increased ROM.
- It appears ligamentum teres injuries occur in the hypermobile, so hip ROM comparison to normals is challenging.
Clinical tests
The Ligamentum Teres test (not shown here) shows high specificity and sensitivity in detecting ligamentum teres pathology. The hip is flexed to 70° then to 30° less than full abduction. The hip is internally and externally rotated in this "open packed" position, with pain indicating a positive result (O'Donnell 2014). Jenny Hynes has amended this, by adding axial compression while rotating, seeming to be more reliable in those hypermobile individuals.
The Log Roll is a clinical test attempting to specifically test ligamentum teres. The test attempts to "wind up" the ligamentum teres then test the degree of elastic recoil. This is demonstrated below.
Chicken or the Egg?
Recent thoughts propose the majority of ligamentum tears are associated with hip microinstability. One article infers ligamentum teres rupture causes increased femoral movement, then causing labral tears and cartilage damage (Phillips, Bartlett, Norton, & Fern, 2012). All other articles suggest that pre-existing bony abnormalities make patients more reliant on passive and dynamic structures, with ligamentous damage occurring once passive structures become overloaded (Cerezal et al., 2012; Martin et al., 2012; Philippon et al., 2012). In those with FAI and hip dysplasia, the ligamentum teres provides additional proprioception and passive restraint.
Impingement or subluxation of the femoral head can occur when repetitive extraphysiological movements are required (such as ballet or kicking sports). Charbonnier and associates, in 2011, found ballet dancers frequently sublux the femoral head, secondary to FAI, even with normal bony anatomy on x-ray and are dependent on stability from ligamentum teres. In those with adequate bony stability, additional passive restraint is not required. In those with hip dysplasia or poor dynamic hip control, passive stability from ligamentum teres is essential, with pathology creating impingement and secondary labral and chondral damage (Charbonnier, 2011).
Imaging
So how do we diagnose ligamentum teres pathology? The correlation between MRI and ligamentum teres damage is poor, with one study finding only 4% of tears were identified on MRI pre-operatively (Botser et al, 2011). MR Arthrograms (a series of MRI's performed after injection of a contrast medium) are often poor, with a study finding only 2 of 23 ligamentum teres ruptures were identified on MR Arthrogram (Bardakos & Villar, 2009). Another study in 2012 compared 116 scans, with radiologists with 10+ years experience diagnosing a maximum of 8 out of 12 tears, however falsely recording up to 26 intact ligaments as having tears, so poor specificity (Blankenbaker, De Smet, Keene, & Del Rio, 2012).
Arthroscopes are the gold standard in detecting ligament pathology. Previously not many arthroscopes reported a ligamentum teres tear (Bardakos & Villar, 2009; Cerezal et al., 2010), but as arthroscopes are becoming more routine, and technology is improving, now 51% of arthroscopes show some damage where previously only full thickness tears were reported (Botser et al., 2011).
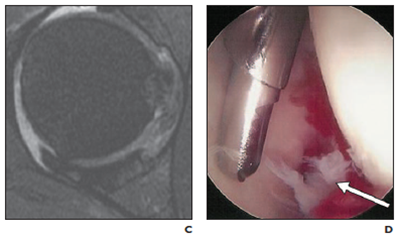
MRI Arthrogram (fraying at 3 o'clock) Arthroscope
Interestingly, the presence of ligamentum teres tears were correlated with increased labral tear size and higher grade chondral damage (p=0.005) than those with intact ligaments (Botser et al., 2011). Another study in 2012 found all full ligamentum teres tears had a co-existing FAI and/or labral damage (Martin et al., 2012). It appears ligamentum teres pathology co-exists with other hip pathology.
Management
There is minimal literature regarding isolated ligamentum teres pathology. Surgical management is performed once conservative management has failed, although the specifics of the conservative management is not described. Haviv, in 2011, debrided 29 ligament stumps with good results, 80% of patients reported full recovery while 20% did not improve and required further surgery. We now have an improved knowledge of hip microinstability, FAI and dysplasia, thanks largely to Joanne Kemp, Leanne Rath and Alison Grimaldi's work, among others. In treating hip instability, impingement and FAI, we are also addressing ligamentum teres overload, causing pathology.
Research on surgical reconstruction has only been undertaken in the past 4 years, with the literature suggesting it is only appropriate in those where instability is greater than pain.
Take Home...
- Ligamentum teres is a pain-producing structure, but is often overshadowed by concurrent pathology (labral and/or chondral pathology), especially in hypermobile individuals with injury occurring secondary to repetitive end-range loading.
- Damage is present in 50% of sporting hip arthroscopies but isolated tears are quite common.
- Currently, the only literature is for surgery, which is recommended after 12 months of failed conservative management.
- As there's no current research on physiotherapy, treatment targets function and return to sport, addressing all impairments.
For further management, read Sian's excellent blogs on Hip Rehab Part A and Part B, which provides a detailed rehabilitation protocol following arthroscope, and can be adapted to address hip impingement and instability.
Alicia
References
Bardakos, N. V., & Villar, R. N. (2009). The ligamentum teres of the adult hip. The Journal of bone and joint surgery. British volume, 91(1), 8-15.
Bedi, A., Kelly, B. T., & Khanduja, V. (2013). Arthroscopic hip preservation surgery: current concepts and perspective. The bone & joint journal, 95-B(1), 10-19.
Blankenbaker, D. G., De Smet, A. A., Keene, J. S., & Del Rio, A. M. (2012). Imaging appearance of the normal and partially torn ligamentum teres on hip MR arthrography. AJR. American journal of roentgenology, 199(5), 1093-1098.
Botser, I. B., Martin, D. E., Stout, C. E., & Domb, B. G. (2011). Tears of the ligamentum teres: prevalence in hip arthroscopy using 2 classification systems. The American journal of sports medicine, 39 Suppl, 117S-125S.
Byrd, J. W. T., & Jones, K. S. (2004). Traumatic rupture of the ligamentum teres as a source of hip pain.
Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association, 20(4), 385-391.
Cerezal, L., Arnaiz, J., Canga, A., Piedra, T., Altonaga, J. R., Munafo, R., & Perez-Carro, L. (2012). Emerging topics on the hip: ligamentum teres and hip microinstability. European journal of radiology, 81(12), 3745-3754.
Cerezal, L., Kassarjian, A., Canga, A., Dobado, M. C., Montero, J. A., Llopis, E., . . . Perez-Carro, L. (2010). Anatomy, biomechanics, imaging, and management of ligamentum teres injuries. Radiographics : a review publication of the Radiological Society of North America, Inc, 30(6), 1637- 1651.
Charbonnier, C., Kolo, F. C., Duthon, V. B., Magnenat-Thalmann, N., Becker, C. D., Hoffmeyer, P., & Menetrey, J. (2011). Assessment of congruence and impingement of the hip joint in professional ballet dancers: a motion capture study. The American journal of sports medicine, 39(3), 557-566.
Gray, A. J., & Villar, R. N. (1997). The ligamentum teres of the hip: an arthroscopic classification of its pathology. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association, 13(5), 575- 578.
Griffiths, E. J., & Khanduja, V. (2012). Hip arthroscopy: evolution, current practice and future developments. International orthopaedics, 36(6), 1115-1121.
Haversath, M., Hanke, J., Landgraeber, S., Herten, M., Zilkens, C., Krauspe, R., & Jager, M. (2013). The distribution of nociceptive innervation in the painful hip: a histological investigation. The bone & joint journal, 95-B(6), 770-776.
Haviv, B., & O'Donnell, J. (2011). Arthroscopic debridement of the isolated Ligamentum Teres rupture. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA, 19(9), 1510-1513.
Kivlan, B. R., Richard Clemente, F., Martin, R. L., & Martin, H. D. (2013). Function of the ligamentum teres during multi-planar movement of the hip joint. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA, 21(7), 1664-1668.
Lindner, D., Sharp, K. G., Trenga, A. P., Stone, J., Stake, C. E., & Domb, B. G. (2013). Arthroscopic ligamentum teres reconstruction. Arthroscopy techniques, 2(1), e21-25.
Martin, R. L., Kivlan, B. R., & Clemente, F. R. (2013). A cadaveric model for ligamentum teres function: a pilot study. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA, 21(7), 1689-1693.
Martin, R. L., Palmer, I., & Martin, H. D. (2012). Ligamentum teres: a functional description and potential clinical relevance. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA, 20(6), 1209-1214.
Petty, N. J. (2011). Principles of neuromusculoskeletal treatment and management : a guide for therapists (2nd ed.). Edinburgh ; New York: Churchill Livingstone Elsevier.
Philippon, M. J., Pennock, A., & Gaskill, T. R. (2012). Arthroscopic reconstruction of the ligamentum teres: technique and early outcomes. The Journal of bone and joint surgery. British volume, 94(11), 1494-1498.
Phillips, A. R., Bartlett, G., Norton, M., & Fern, D. (2012). Hip stability after ligamentum teres resection during surgical dislocation for cam impingement. Hip international : the journal of clinical and experimental research on hip pathology and therapy, 22(3), 329-334.