
San Francisco slopes & stairs slaughter my soleus
Learning by Bob Scher
To learn means to realise something new.
Yet how often do we squint into the unknown through the glare of knowledge,
instead of searching with a beam of ignorance.
Learning never stops. If it does you’re finished.
I’m always in search of more knowledge. Sometimes the aim is to explore a new condition, to understand the latest research trends, or just to refine my current knowledge base. This desire to learn is what drives our blog. In the past 3 months I have been in a new environment, San Francisco. My body has been put under the demand of undulating slopes and stairs and the result is that I’ve experienced several different and new lower limb injuries from plantar fasciitis, patella-femoral joint pain and my calves are generally quite painful & tight.
Pain demands attention.
I know that my calf pain is purely a result of adaptation to a new environment, but I’ve suddenly become inquisitive to understand further “how much the calf muscles are involved in the lower limb kinetic chain” and “if I should be assessing and treating calf tightness more frequently in lower limb injuries (even if the calf is not the source of pain)?”
Anatomy of the calf
Muscle and nerves of the posterior lower limb (Cleland, 2005, p. 294).
Both the gastrocnemius and soleus muscles are responsible for controlling movement into dorsiflexion (as an active restraint). In a task such as squatting, the soleus muscle has to lengthen eccentrically and has an ability to impact DF range more than gastrocnemius, as it is a single-joint muscle (Macrum, et al., 2012).
Gastrocnemius crosses the ankle and knee and is prone to muscle strains with knee extension and ankle dorsiflexion and rapid propulsion. The Soleus is comprised more of slow twitch fibres and only crosses the ankle joint. It is less prone to acute strains but more repetitive strain from walking and stairs.
Kinetic Chain of the lower limb
Here are some fun facts I found about the calf...
At the knee:
Single leg landing technique: ~30% of the control of the anterior shear on the ACL in single leg landing comes from the Soleus muscles. This means that posterior muscles of the lower limb, which don’t cross the knee, still plan a role in control of GRFs. (Mokhtarzadeh, et al., 2013).
I'm sure if I told you that increased hip abduction moments, reduced knee flexion and increased valgus moments are all factors associated with risk of ACL injury during landing, you'd agree. But what if I told you that reduced ankle dorsiflexion range can impact this landing technique further? Both Mauntel et al (2013) and Malloy et al (2014) found a strong association between reduced dorsiflexion and biomechanical changes seen higher in the chain such as increased medial knee displacement. The results of these studies provide evidence to support that calf stretching is a modifiable factor in ACL rehabilitation and for other lower limb injuries with similar maladptive movement patterns.
Macrum et al (2012) explored the relationship between ankle dorsiflexion range and knee kinematics and EMG activity in healthy patients with no history of lower limb injuries. What they found is that reducing the degree of ankle dorsiflexion during a double leg squat (by placing subjects on a wedge which raised them into 12 degrees DF before starting) results in increased soleus EMG activity, reduced EMG activity in vastus lateralis and vastus medialis, a 15% reduction in knee flexion, and an 18% increased knee valgus forces and medial knee displacement. These changes in knee kinematics and muscle activity have been previously associated with patellofemoral joint pain because of the resultant lateral joint loading that occurs during valgus movements during knee flexion.
At the foot & ankle:
Delahunt et al (1998) explored the arthrokinematics and neuromuscular control of the ankle during single leg landing from a drop jump, in patients with functional ankle instability (FI). They presented three main ideas.
The first is that the results indicated that with FI patients demonstrate a lack of pre-initial contact peroneal muscle activity, which is a protective mechanisms to control ankle joint position on impact. As such the ankle will strike at initial contact with increased inversion and also take longer to reach the closed-pack position (CPP) (stable position) of dorsiflexion. This reduced muscle activity leaves the ankle in a vulnerable position and results in increased verticle ground reaction forces and the authors suggest that this is why people with FI are more susceptible to inversion ankle injuries.
A second point discussed in this article is the delayed dorsiflexion caused by reduced eccentric muscle control from the triceps surae (calf muscles). They conclude that a tight calf is also likely to contribute to poor ankle positioning on impact and movement into the CPP and therefore calf stretching should be included in ankle injury rehabilitation.
The third point is that calf muscle length is not the only restraint to ankle dorsiflexion mobility and posterior talar accessory glide should be assessed and restored to normal as soon as position post injury. This PA of the talocrural joint is both a safe and crucial part of initial ankle injury rehabilitation and from my clinical experience, very well tolerated by patients even in the very acute phases.
The demands of slopes and stairs
Leaning the trunk forward during a single leg landing technique moves the centre of mass forward over the knee, which increases the demand on hip extensors, reduces the demand on knee extensors, and increases the demand on ankle plantar flexes. This is good thing for the knee and hip but also needs to be a consideration at the ankle i.e. you need the calf length and control to maintain this posture. Standing more erect moves the centre of mass posteriorly and places more load on the knee (Benke, Powers, & Mandelbaum., 2014). Personally I found that when my calves where very sore and tight I struggled to keep that forward lean position. As a result, I began walking up hills and down stairs with more of an upright trunk and it didn't take long for my knees also became sore.
How do short calves or reduced dorsiflexion make tasks difficult?
Average ankle dorsiflexion range has been documented as 45 degrees in a study exploring risk of ankle injuries in army recruits (Pope, Herbert & Kirwan, 1998). This study reported that reduced ankle dorsiflexion ROM of 34 degree was associated with a 2.5 fold increase in risk of ankle injury, specifically ankle sprains. This association was not found with developing stress fractures and they also provided no significant evidence that pre-activity calf stretching reduces this risk of injury.
A reduction in ankle DF in weight bearing makes it harder to lower our centre of mass. In compensation for this lack of movement, the lower limb will often display more foot pronation, tibial internal rotation, knee valgus and hip internal rotation (Macrum, et al., 2012). This is a pattern of movement we have all seen before. Mostly commonly it prompts me to assess hip and lumbopelvic control but less frequently do I suspect calf length a source of the problem.
Excessive foot pronation has been linked to increased risk of some lower limb injuries such as plantar fasciitis, metatarsal stress fractures, and medial tibial stress syndrome. However, there is a much stronger body of evidence that supports the theory that poor core strength and proximal lumbo-pelvic-hip control are attributing factors in the development of hip and knee injuries (Chuter & de Jong, 2012).
Assessment of dorsiflexion range, and calf length, strength & function

Knee to wall test – measures as distance of toes away from wall or degree of ankle dorsiflexion. This has been shown to be a highly reliable test with very high intra-rater reliability (ICC 0.97-0.99) and inter-rater reliability for both a measurement of distance from the wall (ICC 0.99) and angle of dorsiflexion (ICC 0.97) (Bennell, et al., 1998, p. 175).
The average range of movement of dorsiflexion should be 45-50 degrees or 13-14cm distance from big toe to wall (Bennell, et al., 1998, p. 177). The clinically significant change in range of movement is considered 1-3cm post treatment.
Outcome measures:
- Foot Function Index
- FOAS Foot and Ankle Survey
- Lower extremity functional Scale
- Foot and Ankle Outcome Questionnaire
Palpation:
I try to follow this sequence. Palpate laterally for soleus, centrally through the central tendon/aponeurosis and proximally through muscle belly of med and lat gastroc heads. I also palpate the proximal and distal tibiofibular joints, AP and PA glides at the talocrural joint and follow the tendons all the way into the foot.
Strength assessment of calf muscles with double/single leg calf raise with bent vs straight knee.

Bent knee calf raise above and straight knee right. Check out the difference in tone in my calf muscles. This alone demonstrates how different muscles are active in each position. Give both a go!

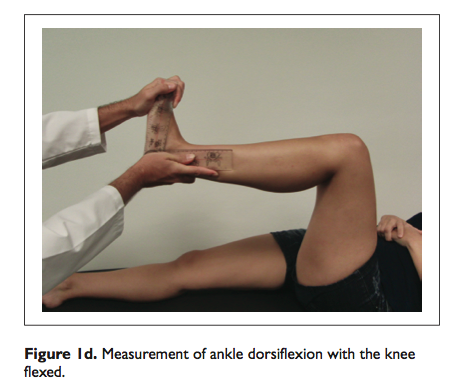
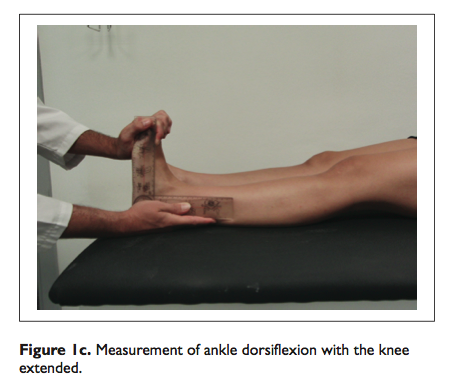
Length assessment:
Ankle dorsiflexion can be measure in weight bearing with the knee to wall lunge but also in non weight bearing as seen below (Bolívar, Munuera, & Padillo, 2013, p. 44). These authors investigated the presence of restricted ankle dorsiflexion range and tightness in muscles in the posterior thigh and leg, in patients with diagnosed plantar fasciitis compared to controls. Restrictions in both the straight leg raise test and ankle dorsiflexion test with knee extension were found to have strong correlations with plantar fasciitis. The straight leg raise test was considered positive is <70 degrees flexion and a sensitivity of 94% and specificity of 82%. Dorsiflexion with knee extension was considered positive if <10 degrees DF and a sensitivity of 96% and specificity of 100%.
Functional assessment - hopping, running, walking and stairs are all important functional movements to observe for both weakness and abnormal movement patterns. Link what you see with what you find on impairment measures.
"Poor proximal neuromuscular control and weakness of hip musculature, in particular the hip abductors and external rotators, lead to poor lower-extremity control in the coronal and transverse planes. As the hip collapses into excessive adduction and internal rotation, the knee falls into dynamic valgus" (Benke, Powers, & Mandelbaum., 2014. p. 52). Continuing down the lower limb, dynamic knee valgus is commonly accompanied with reduced ankle dorsiflexion and increased pronation, which will place undue pressure on structures in the foot and ankle such as the plantar fascia.
These compensations for poor proximal neuromuscular control will overload the knee and ankle and vice versa, limited dorsiflexion and calf length may be the contributing factor to abnormal/increased proximal loading.
When it comes down classification of calf injuries there you can use grades of muscle strain (this is well set out in sports medicine references like Brukner & Khan) but I also really enjoy the classification system present by Mueller-Wohlfahrt and collegues (2012). Particularly with soleus muscle injuries, clinically I've found this are more likely to be non-traumatic overuse injuries or neuromuscular injuries, than acute muscular strains.
Classification and terminology of muscle injuries (Mueller-Wohlfahrt, et al., 2012, p. 4).
Summary
How much are the calf muscles involved in the kinetic chain?
Much more than I thought...
- Reducing the degree of ankle dorsiflexion during a double leg squat by 12 degrees results in increased soleus EMG activity, reduced EMG activity in vastus lateralis and vastus medialis, a 15% reduction in knee flexion, an 18% increased knee valgus forces and medial knee displacement.
- The knee to wall test, dorsiflexion with knee extension and straight leg raise are great tests to evaluate dorsiflexion range of movement as well as muscle tightness.
- There is research linking calf tightness to increased foot pronation and plantar fasciitis, to increase medial knee displacement and dynamic knee valgus seen as contributing factors to both ACL injury risk and PFJS.
- Reduced dorsiflexion and biomechanical changes in the knee also result in pelvic drop and reduced co-contraction of gluteals with hip adductors.
- During landing from a jump, the soleus contributes 30% to the control of anterior knee sheer, which primarily is controlled by the ACL and secondarily by the hamstrings.
Should I be incorporating calves into my assessment of lower limb injuries more frequently?
After finishing this blog my answer is definitely yes!
And just in case you were wondering… I’ve been living in San Francisco for 3 months now and all the pains and injuries I spoke about above have resolved. I stretch more frequently, roll my calves and feet and my legs have adapted to the change. Also, I bought a bike :)
With love from San Francisco from Sian's Soleus
Below are some of the exercises I use to stretch and strengthen my calves.











References
Benke, M. T., Powers, C. M., & Mandelbaum, B. R. (2014). Prevention of Patellofemoral Injuries. In The Patellofemoral Joint (pp. 51-57). Springer Berlin Heidelberg.
Bennell, K., Talbot, R., Wajswelner, H., Techovanich, W., Kelly, D., & Hall, A. J. (1998). Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsiflexion. Australian Journal of Physiotherapy, 44(3), 175-180.
Bolívar, Y. A., Munuera, P. V., & Padillo, J. P. (2013). Relationship between tightness of the posterior muscles of the lower limb and plantar fasciitis. Foot & Ankle International, 34(1), 42-48.
Chuter, V. H., & de Jonge, X. A. J. (2012). Proximal and distal contributions to lower extremity injury: a review of the literature. Gait & posture, 36(1), 7-15.
Delahunt, E., Monaghan, K., & Caulfield, B. (2006). Changes in lower limb kinematics, kinetics, and muscle activity in subjects with functional instability of the ankle joint during a single leg drop jump. Journal of orthopaedic research,24(10), 1991-2000.
Dixon, J. B. (2009). Gastrocnemius vs. soleus strain: how to differentiate and deal with calf muscle injuries. Current reviews in musculoskeletal medicine,2(2), 74-77.
Macrum, E., Robert Bell, D., Boling, M., Lewek, M., & Padua, D. (2012). Effect of limiting ankle-dorsiflexion range of motion on lower extremity kinematics and muscle-activation patterns during a squat. Journal of sport rehabilitation, 21(2), 144.
Malloy, P., Morgan, A., Meinerz, C., Geiser, C., & Kipp, K. (2014). The association of dorsiflexion flexibility on knee kinematics and kinetics during a drop vertical jump in healthy female athletes. Knee Surgery, Sports Traumatology, Arthroscopy, 1-6.
Mauntel, T. C., Begalle, R. L., Cram, T. R., Frank, B. S., Hirth, C. J., Blackburn, T., & Padua, D. A. (2013). The effects of lower extremity muscle activation and passive range of motion on single leg squat performance. The Journal of Strength & Conditioning Research, 27(7), 1813-1823.
Mueller-Wohlfahrt, H. W., Haensel, L., Mithoefer, K., Ekstrand, J., English, B., McNally, S., ... & Ueblacker, P. (2012). Terminology and classification of muscle injuries in sport: a consensus statement. British journal of sports medicine, bjsports-2012.
Mokhtarzadeh, H., Yeow, C. H., Goh, J. C. H., Oetomo, D., Malekipour, F., & Lee, P. V. S. (2013). Contributions of the Soleus and Gastrocnemius muscles to the anterior cruciate ligament loading during single-leg landing. Journal of biomechanics, 46(11), 1913-1920.
Pope, R., Herbert, R., & Kirwan, J. (1998). Effects of ankle dorsiflexion range and pre-exercise calf muscle stretching on injury risk in Army recruits.Australian Journal of Physiotherapy, 44(3), 165-172.