
MCL Rehabilitation- From Ruin to Return to Play
Medial collateral ligament injuries occur following a traumatic valgus force, often while the knee is slightly flexed. Edson (2006) provides a comprehensive overview of the current recommended conservative management of MCL injuries, I highly recommend all physiotherapists read this article. This blog aims to provide a succinct overview of the rehabilitation of MCL injuries, with the approach I use to return an individual to full function.
“Injuries to the medial collateral ligament (MCL) are very common and there seems to be a consensus supporting the conservative management of grade I and II tears. Grade III tears are also usually treated conservatively unless associated with injuries to the anterior cruciate ligament or posterior cruciate ligament.”
Grade I MCL Injury
A grade I (mild) MCL sprain has local tenderness on the medial femoral condyle or medial tibial plateau, with minimal swelling (Brukner & Khan, 2012). There will be pain but no laxity on valgus stress testing at 30 degrees knee flexion. Rehabilitation guidelines are as follows:
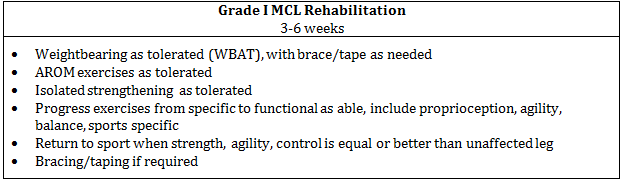
Adapted from Brukner & Khan, 2012 and Edson, 2006
Grade II MCL Injury
A Grade II MCL sprain is caused by a greater valgus stress force. Physical findings include marked tenderness over the MCL, mild to moderate swelling and pain and laxity on valgus stress testing. The knee should be stable at full extension, with laxity only present at 30 degrees flexion. Rehabilitation guidelines are as follows:
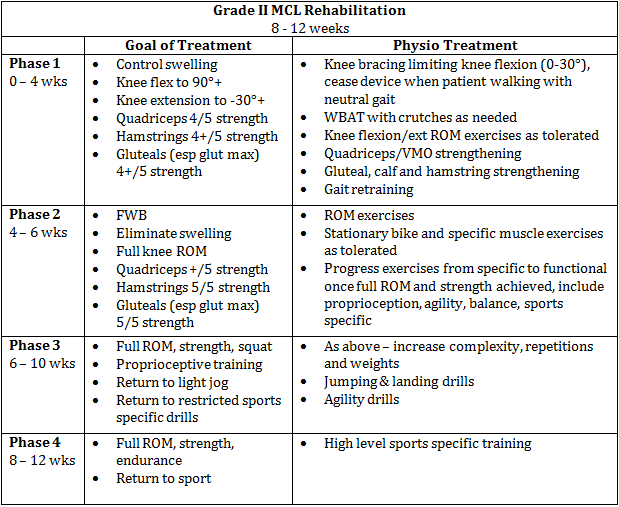
Adapted from Brukner & Khan, 2012 and Edson, 2006
Grade III MCL Injury
A grade III sprain is complete rupture of the ligament, resulting from severe valgus force. On examination, there is tenderness over the MCL, with severe laxity on valgus stress testing without a distinct end-feel. There could also be laxity at full extension, indicating damage to the deeper, capsular fibres of the MCL. There may be minimal pain on testing, due to rupture of nociceptive fibres. There is rarely an associated medial mensicus injury, instead lateral meniscus is more involved due to the mechanism of injury, compressing and shearing the lateral compartment while opening the medial compartment (Brukner & Khan, 2012). Rehabilitation guidelines are as follows:
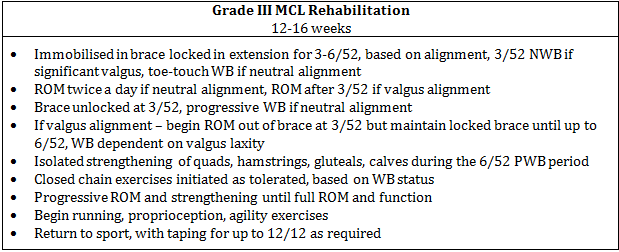
Adapted from Edson, 2006
Strengthening Exercises
The following exercises are often included in my rehabilitation programs. I find the most important part of the exercise is the cueing, to ensure correct muscle activation and motor patterning. I regularly ask the patient, "Where do you feel that?" to ensure the patient is isolating and targeting the desired muscles. The focus of my rehabilitation is to regain neutral joint alignment, which requires strength and endurance of VMO, gluteus maximus and medial gastrocnemius. This focus is largely influenced by Michael Vadiveloo, FACP. I have included some common exercises and the words I use to achieve this correct muscle activation.

VMO Wall Sit
VMO Wall Sit
- "feet shoulder width apart, feet facing forwards, knees at 90 degrees, weight on inside of heels, turn your knees out"
- weight on inside of heels = VMO bias
- Hold up to 60 seconds, progress by moving unaffected leg further from wall, increase WB on MCL leg

Bridge

Modified Bridge

Single Leg Bridge
Bridge
- "feet shoulder width, toes facing forwards, push through heels, push hips off, relax your back/abs"
- weight on heel = glut max bias
- 20 reps, progress to Modified Bridge
Modified Bridge
- "one foot further out, push through closest heel, squeeze your butt, push your hips up"
- weight on heel, knee out = glut max bias
- 20 reps/leg, progress to SL Bridge
Single Leg Bridge
- "push through your heel, squeeze your butt, push your hips up, relax your back/abs"
- glut max bias
- 20 reps/leg, as soon as you feel hamstrings/back/quads kicking in, revert back to modified bridge, should feel only glut max!!

Squat
Squat
- "feet shoulder width apart, feet facing forwards, weight on your heels, turn your knees out, sit behind you, push up through your heels"
- glut max and VMO bias, neutral knee alignment
- 20 reps, progress with adding weights/reducing stability (lunge, single leg)

Lunge
Lunge
- "keep shin vertical, weight on front heel, turn your knee out, drop your hips straight down, push up through your front heel"
- VMO and glut max bias
- 20 reps/leg, progress with adding weights or Bulgarian Lunge

Bulgarian Lunge
Bulgarian Lunge
- "foot facing forwards, weight on front heel, turn your knee out, keep hips level, sit back behind you, push up through front heel"
- glut max bias
- 20 reps/leg, progress by adding weights or Arabesque

Arabesque Hold - Hands Supported

Arabesque Unsupported / Arabesque Squat
Arabesque
- "arms out in front, back flat, foot facing forwards, sit back on your heel, turn your knee out, hold"
- glut max bias
- Hold 60 secs/leg, progress to Leg Supported then Unsupported then Arabesque Squat
Arabesque Squat
- "as above...sit behind you bending your knee, push up through your heel"
- glut max and VMO bias
- 20/leg, stop when glutes fatigue or when hamstrings kick in, ensure only feel glutes
My program would also include hamstring curls, straight leg bridging, Romanian dead lifts and calf raises, to facilitate calf and hamstring strengthening.
These exercises are used in Phases I and II of MCL rehabilitation, further exercises for sports specific, proprioception, agility and power exercises will be described in a future blog. For further information, I encourage you to read Edson, 2006, and Brukner & Khan, 2012. Both provide excellent summaries of MCL rehabilitation, especially the progressions and goals for each stage of rehab. Brukner & Khan, in particular, show various alternative exercises for rehabilitation, which may also be beneficial.
In summary, the focus of the rehabilitation is to ensure the correct muscle activation and joint alignment throughout any exercise. The chosen exercise isn't important, as long as the patient feels the muscle working in the correct area.
Alicia
References
Brukner, P., & Khan, K. (2012). Brukner & Khan's clinical sports medicine (4th ed.). Sydney ; New York: McGraw-Hill.
Edson, C. J. (2006). Conservative and postoperative rehabilitation of isolated and combined injuries of the medial collateral ligament. Sports medicine and arthroscopy review, 14(2), 105-110.