
Frozen Shoulder...Fear Avoidance?
Introducing Rex...
- 63 year old male with (R) shoulder pain, gradual insidious onset 5 months ago
- Shld pain = constant 4/10 ache with 9/10 sharp pain on >90° elevation
- Aggs – “any movement”, clothes on line, washing hair, arm out to side, using computer
- Eases – doing nothing
- PM – unable to sleep on (R)shoulder, sleeps 3-4 hrs max at a time
- HPC: 2 hydrodilatations (R) shld in past 4/12
- PMH: (L) adhesive capsulitis 17 yrs ago, 2x hydrodilatations (L) shld
- SHx: unemployed, lives in share house, does own cooking, cleaning, walks daily
- Goals – “fix the shoulder”, get surgery as nothing has worked
Physical Examination
- (R) Shld flex, abd’n = <100° R2 P8/10
- HBB = L5
- (R) GHJ AP hypo++ P4/10
- TrP (R) infraspinatus P9/10 referral to (R) Cx & down arm
- (R) Empty/Full can at 60° = P7/10
- ER strength (R) =4/5

Photo courtesy of google images
Day One Treatment
- AP (R) GHJ in 45° abd’n mobs IV ++ 3x60s // (R) shldflex 150° R2 P7/10 (↑50°), (R) abd’n 120° R2 (↑ 25°)
- HEP – Active assisted shld flexion
Four days later…(R) shld flex 160°, abd’n 150°
SURELY NOT??
Given Rex’s issue was a capsular thickening with chronic inflammation, is it possible to get a 60° increase in shoulder flexion in 4 days, even following a hydrodilatation?? Was his restriction pure stiffness or apprehension/pain restriction? Did Rex’s beliefs about pain and his behaviour since injury affect his recovery?
To explore this further, I have included current models of pain related fear and fear avoidance.
Fear Avoidance Model
In 1983 Lethem proposed a model describing avoidance of a movement or activity due to fear of pain. An injury causes a sympathetic nervous system response including anxiety and fear, the patient then associates activity with the nervous response resulting in conditioning. The patient begins to predict pain when an activity occurs, causing the avoidance of an activity or situation to avoid the fear and anxiety response (Vlaeyen 2000).
Downward spiral
- Negative thoughts/appraisals of pain - catastrophise
- Fear causes avoidance/escape - ADL’s not accomplished
- Avoidance based on anticipation of pain so less chances to correct/realise own behaviour & beliefs
- Long term avoidance can affect musculoskeletal/cardio systems causing “disuse syndrome”
- Become hypervigilant, more focused on pain, less able to divert attention
- Pain-related fear associated with increased psychological responses, increased reaction to ‘dangerous situation’ (Vlaeyen 2000)
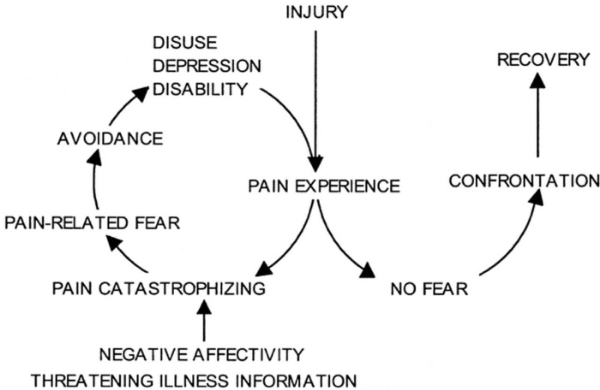
Vlaeyen (2000)
Pain Related Fear
Patients begin to overpredict pain levels (predict higher levels and earlier in ROM). In trying to escape from/avoid a perceived threat they gradually avoid P1, causing their daily activity to decrease and reduced daily function. A study by Crombez (1999) found pain-related fear was a better predictor than pain intensity on a trunk flexion/extension weight lifting task. Pain-related fear is a better indicator of patient disability levels than medical findings or pain intensity (Vlaeyan 2000).
Disuse Syndrome
Prolonged avoidance of activity results in detrimental changes to the musculoskeletal system, deconditioning occurs causing a change in muscle tone and activation levels. Patients display guarded movement: a change in motor patterning, altered activation and co-contraction on certain movements (Vlaeyen 2000).
Did my treatment just address Rex’s muscle activation and reduce guarding? How many pts with adhesive capsulitis avoid movement with gradual reduction in function? Initially described for chronic low back pain (LBP), could it be relevant to the shoulder also??
Fear Avoidance in the Shoulder?
- Van der Windt 2007 – compared psych factors in shoulder & LBP
- Found fear-avoidance questionnaire results were close at baseline (58 shoulder vs 62 LBP), after 3/12 shoulder Fear Avoidance Behaviour Questionnaire (FABQ) had reduced drastically
- Shoulder patients often see physios in first 3/12 of shoulder pain, are we accidentally treating behaviours?
- George 2011 – assessed pain-related fear in Lx, Cx, shoulder, knee
- High pain-related fear beliefs had higher pain & lower function at baseline in all four areas, not strictly a low back pain model
- George 2007 – effect of DOMS on shoulder outcomes
- Fear of pain predicted pain levels
- Fear of pain & pain intensity predicted disability
- Anxiety and pain catastrophising had no effect on shoulder outcomes
- Sindhu 2012 – assessed effect of fear-avoidance on shoulder rehab
- Elevated fear-avoidance beliefs had poorer functional outcomes only in muscle/tendon/soft tissue group (54% of shoulder patients)
- No effect in the post-surg, arthropathy, fracture, sprain/strain groups
- Possibly being given a clear, structural/anatomical diagnosis reduced fear??
Assessment of Pain Related Fear
- Fear of Pain Questionnaire (FPQ) (McNeil 1998)
- 30 questions, detects high and low fear-of-pain patients
- Tampa Scale for Kinesiophobia (TSK-11)
- Shorter measure for fear of movement, valid and reliable in clinical setting (Woby 2005, Tkachuk 2012)
- Pain Anxiety Symptoms (PASS)
- Good reliability and validity in research in clinical setting (McCracken 1992, Burns 2000, Coons 2012)
- Fear-Avoidance Beliefs Questionnaire (FABQ) (Waddell 1993)
- Mintken 2010 - changed ‘back’ to ‘shoulder’, strong indicator of FAB/PRF, strong correlation to SPADI
- Inrig 2012 assessed FABQ in worker’s compensation patients, poor correlation as high ceiling effect
Rex
So in Rex's case, he had restricted shoulder AROM (flex, abd, HBB, ER) but was that pure capsular restriction or apprehension? Given he had received two hydrodilatations in the past four months, and had such a drastic improvement after grade III mobilisations, it is more realistic to attribute his restriction to pain apprehension and disuse. His pain experience was heightened, he avoided painful movements and had five months of shoulder neglect. This case study taught me fear avoidance is applicable to all injuries, not only low back pain, with the mind being a very powerful contributor to clinical symptoms. In future, I would use a fear/pain questionnaire alongside a shoulder pain and disability index (SPADI) to determine the factors of the patient's pain.
For Rex, we spent a lot of time discussing the fear, constantly highlighting the clinical improvements, then gradually increasing the stimulus at the shoulder. The patient was given a pain-free home exercise program to increase compliance and reduce fear avoidance.
Clinical Implications
- Assess their fear – FPQ, PASS, TSK-11
- Address their fear – education, show patient the changes
- “Patient views his pain as a common condition that can be self-managed, rather than as a serious disease or a condition that needs careful protection.” Vlaeyen 2000, pg 328.
- “It is far more convincing to actually experience him/herself behaving differently than it is to be told that he/she is capable of behaving differently” Vlaeyen 2000, pg 329.
- Graded exposure to fearful activity/stimulus
- Crombez 1999 found although higher initial pain response, with graded exposure to painful activity, fear decreased & ROM increased rapidly
- Bailey 2009 found graded exposure and acceptance & commitment therapy most effective in treating fear-avoidance in chronic musc pain
- Greater focus on function than pain intensity
- “Treatment strategies should focus on improving functional abilities… using a small-steps approach…thus enhancing self-efficacy and reducing fear.” (Denison 2004, pg 251)
Alicia
References
Bailey, K. M., Carleton, R. N., Vlaeyen, J. W. S., & Asmundson, G. J. G. (2010). Treatments addressing pain-related fear and anxiety in patients with chronic musculoskeletal pain: a preliminary review. Cognitive behaviour therapy, 39(1), 46-63.
Burns, J. W., Mullen, J. T., Higdon, L. J., Wei, J. M., & Lansky, D. (2000). Validity of the pain anxiety symptoms scale (PASS): prediction of physical capacity variables. Pain, 84(2-3), 247-252.
Coons, M. J., Hadjistavropoulos, H. D., & Asmundson, G. J. G. (2004). Factor structure and psychometric properties of the Pain Anxiety Symptoms Scale-20 in a community physiotherapy clinic sample. European journal of pain (London, England), 8(6), 511-516.
Crombez, G., Vlaeyen, J. W., Heuts, P. H., & Lysens, R. (1999). Pain-related fear is more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain, 80(1-2), 329-339.
Denison, E., Asenlof, P., & Lindberg, P. (2004). Self-efficacy, fear avoidance, and pain intensity as predictors of disability in subacute and chronic musculoskeletal pain patients in primary health care. Pain, 111(3), 245-252.
George, S. Z. (2006). Fear: a factor to consider in musculoskeletal rehabilitation. The Journal of orthopaedic and sports physical therapy, 36(5), 264-266.
George, S. Z., Dover, G. C., & Fillingim, R. B. (2007). Fear of pain influences outcomes after exercise-induced delayed onset muscle soreness at the shoulder. The Clinical journal of pain, 23(1), 76-84.
George, S. Z., & Stryker, S. E. (2011). Fear-avoidance beliefs and clinical outcomes for patients seeking outpatient physical therapy for musculoskeletal pain conditions. The Journal of orthopaedic and sports physical therapy, 41(4), 249-259.
George, S. Z., Wallace, M. R., Wright, T. W., Moser, M. W., Greenfield, W. H., 3rd, Sack, B. K., . . . Fillingim, R. B. (2008). Evidence for a biopsychosocial influence on shoulder pain: pain catastrophizing and catechol-O-methyltransferase (COMT) diplotype predict clinical pain ratings. Pain, 136(1-2), 53-61.
Inrig, T., Amey, B., Borthwick, C., & Beaton, D. (2012). Validity and reliability of the Fear-Avoidance Beliefs Questionnaire (FABQ) in workers with upper extremity injuries. Journal of occupational rehabilitation, 22(1), 59-70.
Leeuw, M., Goossens, M. E. J. B., Linton, S. J., Crombez, G., Boersma, K., & Vlaeyen, J. W. S. (2007). The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. Journal of behavioral medicine, 30(1), 77-94.
Lentz, T. A., Barabas, J. A., Day, T., Bishop, M. D., & George, S. Z. (2009). The relationship of pain intensity, physical impairment, and pain-related fear to function in patients with shoulder pathology. The Journal of orthopaedic and sports physical therapy, 39(4), 270-277.
Moseley, L G. (2011). A new direction for the fear avoidance model? Pain, 152(11), 2447-2448.
McCracken, L. M., Zayfert, C., & Gross, R. T. (1992). The Pain Anxiety Symptoms Scale: development and validation of a scale to measure fear of pain. Pain, 50(1), 67-73.
McNeil, D. W., & Rainwater, A. J., 3rd. (1998). Development of the Fear of Pain Questionnaire--III. Journal of behavioral medicine, 21(4), 389-410.
Mintken, P. E., Cleland, J. A., Whitman, J. M., & George, S. Z. (2010). Psychometric properties of the Fear-Avoidance Beliefs Questionnaire and Tampa Scale of Kinesiophobia in patients with shoulder pain. Archives of physical medicine and rehabilitation, 91(7), 1128-1136.
Sindhu, B. S., Lehman, L. A., Tarima, S., Bishop, M. D., Hart, D. L., Klein, M. R., . . . Wang, Y.-C. (2012). Influence of fear-avoidance beliefs on functional status outcomes for people with musculoskeletal conditions of the shoulder. Physical therapy, 92(8), 992-1005.
Tkachuk, G. A., & Harris, C. A. (2012). Psychometric properties of the Tampa Scale for Kinesiophobia-11 (TSK-11). The journal of pain : official journal of the American Pain Society, 13(10), 970-977.
van der Windt, D. A. W. M., Kuijpers, T., Jellema, P., van der Heijden, G. J. M. G., & Bouter, L. M. (2007). Do psychological factors predict outcome in both low-back pain and shoulder pain? Annals of the rheumatic diseases, 66(3), 313-319.
Vlaeyen, J. W., & Linton, S. J. (2000). Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain, 85(3), 317-332.
Vlaeyen, J. W. S., & Linton, S. J. (2012). Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain, 153(6), 1144-1147.
Waddell, G., Newton, M., Henderson, I., Somerville, D., & Main, C. J. (1993). A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain, 52(2), 157-168.
Woby, S. R., Roach, N. K., Urmston, M., & Watson, P. J. (2005). Psychometric properties of the TSK-11: a shortened version of the Tampa Scale for Kinesiophobia. Pain, 117(1-2), 137-144.