
Pelvic girdle pain - which test to choose?

The second part of this blog explores the differential diagnosis for PGP, the large battery of tests which current exist and how the cumulative information from these assessments can assist our clinical reasoning and diagnostic classification of PGP.
If you missed it, the previous blog provided an introduction into the dissection of this clinical practice guideline and explored the prevalence and presentation of pelvic girdle pain in the antepartum population.
Differential diagnosis
Currently there remains a lack of consensus around the diagnostic pathway for determining PGP and there is no gold standard (Vleeming, et al., 2009, p. 804). Physical Therapists need to consider many different elements during their diagnosis and classification:
- Are you able to distinguish between low back pain compared to pelvic girdle pain?
- If you feel that the pain location and behaviour is pointing towards PGP, are you able to further differentiate symptoms into location (pubic symphysis, left SIJ, right SIJ or the entire pelvic girdle) or, are you able to use non-specific functional category such as reduced/excessive force or form closure?
- Is there any involvement from the hip (it is important to rule our femoral neck stress fractures)?
- Are there any contributing psychosocial factors - how might you screen and identify these?
- Are there any other medical conditions that could be mimicking this condition (urinary or gynecological conditions, systemic inflammatory joint disorders, femoral neck stress fractures, or cancer)?
Clinton et al (2017, p.110) suggest that therapists "should proceed with caution and consider medical referral for any history of":
- Trauma,
- Unexplained weight loss,
- History of cancer,
- Steroid use,
- Drug abuse,
- Human immunodeficiency virus or immunosuppressed state,
- Neurological symptoms/signs,
- Fever, and/or systemically unwell,
- Referred pain due to urinary tract infection to the lower abdomen/ pelvic or sacral region,
- Failure to achieve functional improvement,
- Pain that does not reduce with rest.
Taking a thorough history involves noting the:
- Pain location, pain intensity, pain pattern, pain behaviour with postures
- Levels of disability or impairment
- Specific history relating to PGP
- Family history of PGP
- Patient’s beliefs about pain and recovery and their active coping strategies
- Presence of fear avoidant behaviour or on the converse, pacing issues
- Concurrent disorders - incontinence, sexual dysfunction
Clinical assessment
There are many tests that current exist for therapists to use in the assessment of PGP. I have always been taught to use a cluster of tests as this improves the reliability and validity of the results. There is no single gold standard measure for this diagnosis and therapists need to look at an array of measures.
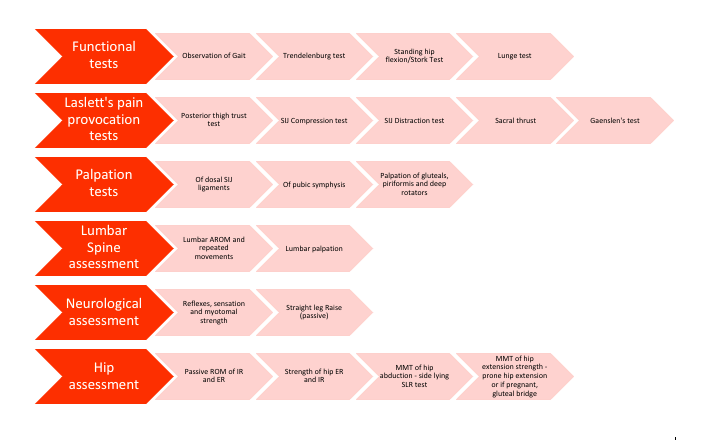
My clinical preference for directing assessment of PGP.
The CPG goes looks at each test individually and provides a thorough description of how the test should be performed, what it measures and the psychometric properties of each test in isolation. Clinton et al (2017) shared these values from Cook et al (2007), which is a hallmark paper that looked at the combined properties of using these tests in as a cluster. Cook et al (2007) found that when combined;
- The lunge, ASLR and PPT have a sensitivity of 0.94 and specificity of 0.66.
- The ASLR, Gaenslen’s and PPT with a sensitivity of 0.88 and specificity of 0.66.
- The lunge, MTT of the hip and hip PROM combined together have a sensitivity of 0.7 and specificity of 0.83.
- What we can take away from these results is that combining several tests will provide you with the most valuable information!

One of my favourite active tests (the active straight leg raise) is commonly used in this assessment protocol and has been previously described in detail here.
The paper by Cook et al (2007) is the same paper that I was taught with to understand the combined value of these test, however I was then taught to create a much larger assessment for the differentiation between LBP and PGP, which I have represented in the flowchart above. Throughout this examination during the functional tests, lumbar spine assessment and observation of limited activities, the clinician needs to pay careful attention to the movement patterns being demonstrated in the hopes of identifying maladaptive movement patterns contributing to peripheral-mediated non-specific PGP.
Outcome measures
A common generalized disability outcome measure is the disability rating index, which is not population specific to PGP. This is a rating scale that asks patients to describe the level of difficulty they have with dressing, walking outdoors, climbing stairs, sitting, bending forward, making beds, carrying a bag, running, light work, heavy work, lifting heavy objects, sporting activities. Not one that I use for this patient population.
The Oswetry Disability Index and Roland-Morris Disability Questionnaire have been validated across LBP including the antepartum population - again these are back-pain specific questionnaires.
“The PGQ is currently the only outcome measure specifically developed to evaluate impairments and functional limitations of PGP during pregnancy and postpartum. The PGQ was developed to include questions from the DRI, ODI, and RMDQ, as well as functional activity questions that were considered clinically relevant by clinicians and a patient focus group. The PGQ is simple to concurrently administer with fear and catastrophization outcomes measures.” (Clinton, et al., 2017, p.112).
Other outcome measures to consider are the Fear Avoidance Beliefs Questionnaire and the Pain Catastrophisation Scale. I’ve previously explored the use of these two questionnaires in the assessment of a patient with PGP and LBP and specifically highlighted how they altered my treatment direction. You can read more about that here.
Classification
An interesting point to note is that most papers emphasise how important the examination is in diagnosis, yet barely none help the clinician understand the specific requirements of this examination. I’ve always referred to the masterclass by O’Sullivan & Beales (2007) to guide my clinical practice. What I really like about the masterclass published by O’Sullivan and Beales in 2007 is that they helped interpret the findings of examination and provide a categorisation of pain as seen below (O’Sullivan & Beales., 2007a, p.90).
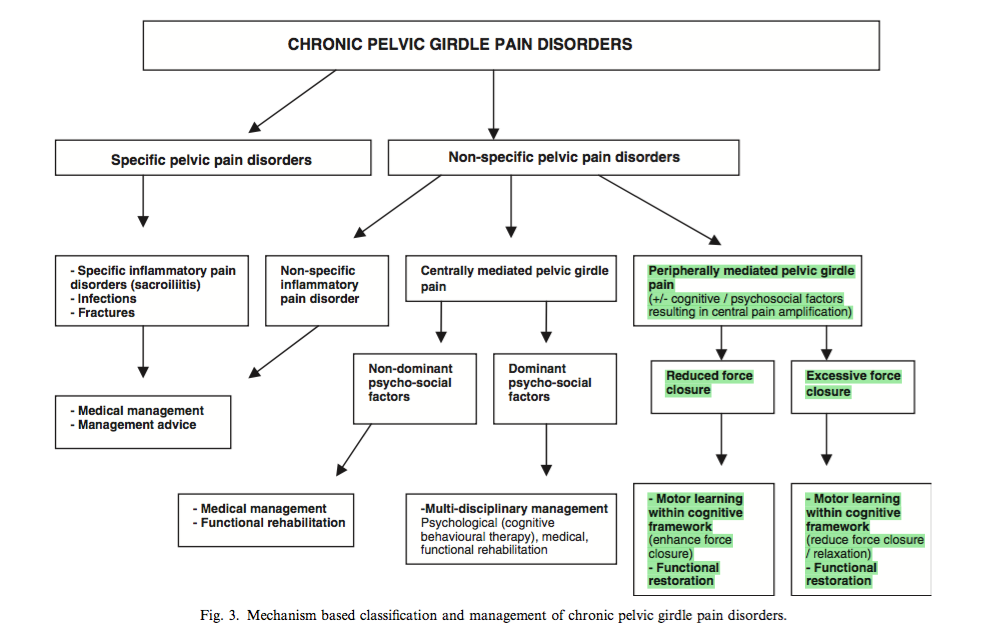
Clinical reasoning pathway (O’Sullivan & Beales., 2007a, p.90)
Following the history and physical examination, the therapist will aim to classify the patient has having a specific or non-specific pelvic girdle pain disorder. Specific PGP disorders often include conditions that we consider under red flags eg: systemic inflammatory conditions, infections or fractures, all of which require medical attention foremost before exploring the role of physiotherapy. In generally, physiotherapy can be limited in effectiveness for specific PGP. The second group, non-specific PGP can be further divided into centrally-mediated and peripherally-mediated pain disorders. This is where implementing different outcome measures during your clinical examination can be very helpful in identifying psychologically-mediated pain disorders. The conditions we are most interested in treating are the non-specific PGP disorders with peripherally mediated mal-adaptive motor control impairments which represent the driving mechanism for PGP. These motor control impairments come under the term reduced/excessive force closure and are managed with education, functional reeducation, and therapeutic exercise to either reduce the excessive muscle activation or promote further stability to enhancing the motor control effect of local pelvic muscles. The important thing to note is that these muscles are not generally trained in isolation, but rather as part of a movement-retraining functional approach.
Next up, we look at the interventions recommended for the treatment of PGP through the clinical practice guideline published by Clinton et al (2017).
Sian
References:
Albert, H., Godskesen, M., & Westergaard, J. (2000). Evaluation of clinical tests used in classification procedures in pregnancy-related pelvic joint pain. European Spine Journal, 9(2), 161-166.
Albert, H. B., Godskesen, M., & Westergaard, J. G. (2002). Incidence of four syndromes of pregnancy-related pelvic joint pain. Spine, 27(24), 2831-2834.
Bjorklund, K., Bergstrom, S., Nordstrom, M. L., & Ulmsten, U. (2000). Symphyseal distention in relation to serum relaxin levels and pelvic pain in pregnancy. Acta obstetricia et gynecologica Scandinavica, 79(4), 269-275.
Clinton, S. C., Newell, A., Downey, P. A., & Ferreira, K. (2017). Pelvic Girdle Pain in the Antepartum Population: Physical Therapy Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Section on Women's Health and the Orthopaedic Section of the American Physical Therapy Association. Journal of Women's Health Physical Therapy, 41(2), 102-125.
Cook, C., Massa, L., Harm-Ernandes, I., Segneri, R., Adcock, J., Kennedy, C., & Figuers, C. (2007). Interrater reliability and diagnostic accuracy of pelvic girdle pain classification. Journal of Manipulative & Physiological Therapeutics, 30(4), 252-258.
Franklin, M. E., & Conner-Kerr, T. (1998). An analysis of posture and back pain in the first and third trimesters of pregnancy. Journal of Orthopaedic & Sports Physical Therapy, 28(3), 133-138.
Gutke, A., Östgaard, H. C., & Öberg, B. (2008). Association between muscle function and low back pain in relation to pregnancy. Journal of rehabilitation medicine, 40(4), 304-311.
Hungerford, B., Gilleard, W., & Hodges, P. (2003). Evidence of altered lumbopelvic muscle recruitment in the presence of sacroiliac joint pain. Spine, 28(14), 1593-1600.
Hungerford, B., Gilleard, W., & Lee, D. (2004). Altered patterns of pelvic bone motion determined in subjects with posterior pelvic pain using skin markers. Clinical biomechanics (Bristol, Avon), 19(5), 456-464.
Mens, J. M., Pool-Goudzwaard, A., & Stam, H. J. (2009). Mobility of the pelvic joints in pregnancy-related lumbopelvic pain: a systematic review. Obstetrical & gynecological survey, 64(3), 200-208.
Mens, J. M., Huis, Y. H., & Pool-Goudzwaard, A. (2012). Severity of signs and symptoms in lumbopelvic pain during pregnancy. Manual therapy, 17(2), 175-179.
Mens, J. M., Vleeming, A., Snijders, C. J., Koes, B. W., & Stam, H. J. (2001). Reliability and validity of the active straight leg raise test in posterior pelvic pain since pregnancy. Spine, 26(10), 1167-1171.
Mens, J. M., Vleeming, A., Snijders, C. J., Koes, B. W., & Stam, H. J. (2002). Validity of the active straight leg raise test for measuring disease severity in patients with posterior pelvic pain after pregnancy. Spine, 27(2), 196-200.
Mens, J. M. A., Snijders, C. J., & Stam, H. J. (2000). Diagonal trunk muscle exercises in peripartum pelvic pain: a randomized clinical trial. Physical therapy, 80(12), 1164-1173.
Nascimento, S. L., Surita, F. G., & Cecatti, J. G. (2012). Physical exercise during pregnancy: a systematic review. Current Opinion in Obstetrics and Gynecology, 24(6), 387-394.
O’Sullivan, P. B., Beales, D. J., Beetham, J. A., Cripps, J., Graf, F., Lin, I. B., ... & Avery, A. (2002). Altered motor control strategies in subjects with sacroiliac joint pain during the active straight-leg-raise test. Spine, 27(1), E1-E8.
O'Sullivan, P., & Beales, D. (2007a). Diagnosis and classification of pelvic girdle pain disorders--Part 1: a mechanism based approach within a biopsychosocial framework. Manual therapy, 12(2), 86-97.
O'Sullivan, P., & Beales, D. (2007b). Diagnosis and classification of pelvic girdle pain disorders, Part 2: illustration of the utility of a classification system via case studies. Manual therapy, 12(2), e1-12.
Vleeming, A., Albert, H. B., Östgaard, H. C., Sturesson, B., & Stuge, B. (2008). European guidelines for the diagnosis and treatment of pelvic girdle pain. European Spine Journal, 17(6), 794-819.
Vleeming, A., Schuenke, M. D., Masi, A. T., Carreiro, J. E., Danneels, L., & Willard, F. H. (2012). The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. Journal of anatomy, 221(6), 537-567.
Vleeming, A., Stoeckart, R., Volkers, A. C., & Snijders, C. J. (1990). Relation between form and function in the sacroiliac joint. Part I: Clinical anatomical aspects. Spine, 15(2), 130-132.
Vøllestad, N. K., & Stuge, B. (2009). Prognostic factors for recovery from postpartum pelvic girdle pain. European spine journal, 18(5), 718-726.