
Variations in Squat Technique
Today I read this fantastic (and funny) article on why we should squat more which highlighted one of my biggest challenges as a clinical pilates instructor, teaching people how to squat.
The author emphasised in Western Society people forget how to squat (because they don't need to in everyday function) and then over time, their bodies become deconditioned and lose the ability to squat as well.

"The squat is a widely used exercise that activates the largest, most powerful muscles in the body and may be the greatest test of lower-body strength. The major muscles involved are the quadriceps, hamstrings, gastrocnemius, and the gluteus maximus. The squat also relies on muscle activity at both the hip and ankle joints and recruits the abdominals and spinal erectors as well" (Gullett, Tillman, Gutierrez, & Chow., 2009, p.284).
Squatting is defined in power lifting as the movement where a person lowers their body by bending their knees and hips, until the hips have dropped below the line of the knees, and then ascends to an upright position of full knee and hip extension (Escamilla, Fleisig, Lowry., et al, 2001). As a compound closed-chain exercise, it is a critical clinical rehabilitation tool.
"Squats are considered one of the most functional and efficient weight-bearing exercises" (Gullett, Tillman, Gutierrez, & Chow., 2009, p. 284).
"The attractiveness of this exercise lays in the fact that no specialized equipment is required for performance, the physical space necessary for carrying out the movement in relatively small, the exercise resembles the performance of several everyday tasks, and several simple modifications may be made to affect training dosage and intensity" (Almosnino, Kingston & Graham., 2013, p. 33).
How do we pick the best squatting exercise for our clients?
When prescribing a squat to your client, these variables must all be considered: squat depth, stance width, foot rotation, bar position, joint compression and exercise variations.
Squat depth
- Schoenfeld (2012), among many others, categorises squat depth into the following:
- Partial squat (0-40 degrees knee angle)
- Parallel squat (hips parallel to knees or 70-100 degrees knee angle)
- Deep squat (full range or >100 degrees knee angle)
- If work-outs are focused on maximal force or power, then partial squats are more effective than parallel squats. If the goal is to increase work performance, parallel or deep squats should be considered, as half as many repetitions are required to provide the same conditioning (Drinkwater, Moore, & Bird., 2012).
- There is little variation in activity between biceps femoris, vastus lateralis and vastus medialis between partial, parallel and full squats. Gluteus maximus was found to have the greatest variation in contribution during the concentric phase for a partial (26%), parallel (27%) and full squat (40%) (Caterisano, Moss, Pellinger, Woodruff, et al., 2002). This research suggests that gluteus maximus activity increases more than bicep femoris activity as squat depth increases, during a weight back squat.
Stance width
- Escamilla, Fleisig, Lowry, and colleagues (2001) found:
- Plantar flexor muscles will work harder in narrow stance, while dorsiflexor muscles will work harder in normal and wide stance.
- Hip and knee extensors will work harder in normal and wide stance, especially below 45 degrees of knee flexion.
- Narrow stance has greater knee shearing forces than normal and wide stance .
- 'During a back squat, the modification of the stance width does not influence the EMG activity of thigh muscles (VL, VM, RectFem, Semiten, BFem, gluteus medius, and the adductors), with exception of gluteus maximus' ( Paoli, Marcolin & Petrone., 2009).
- Paoli and colleagues (2009) found that EMG values of gluteus maximus were greater with wide stance (140% of shoulder width) and during loads of 75% 1RM.
Foot rotation
Almosnino, Kingston & Graham (2013) assessed the effect of stance width and foot rotation on 3-D knee movements (flexion, extension, abduction, adduction, internal rotation, and external rotation). Like many previous studies, the authors were unable to find a clinically significant difference between stance positions and foot rotation. They concluded that variation in rotation is purely for patient comfort.
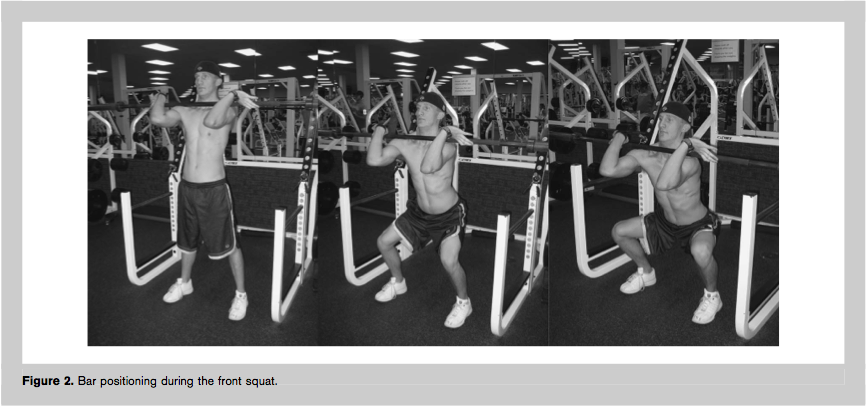
Front squat versus back squat
"Although bar position did not influence muscle activity, muscle activity was significantly different between the ascending and descending phases. The front squat was shown to be just as effective as the back squat in terms of overall muscle recruitment, with significantly less compressive forces on the knee" (Gullett, Tillman, Gutierrez, & Chow., 2009, p.291). The authors also found no difference in shearing forces on the knee between front and back squat.

(Gullett, Tillman, Gutierrez, & Chow., 2009, p. 285)
(Gullett, Tillman, Gutierrez, & Chow., 2009, p. 285)
Joint compressive forces.
Escamalli and colleagues (2009) investigated patellofemoral joint compressive loads during a wall squat with feet close to the wall (short) and far from the wall (long), and compared to a single leg squat, with the following findings. Firstly, in all positions the joint compressive forces are highest between 70-90 degrees knee flexion, with the wall squat short causing the most compression. This is hypothesised to result from increased forward translation of the knee over the foot. Secondly, there are less compressive loads in a single leg squat compared to short wall squat, possibly due to a change of centre of mass and increased hamstring activity on a trunk forward lean during the single leg squat.
"With deep squats often listed as a contraindicated exercise, it is not unusual for many coaches and trainers to believe that this contraindication applies to all squatting movements. No research has ever shown that parallel squats create high shearing force through the knee. Parallel squats are not only safe when performed correctly but are an integral part of effective fitness training programs" (Drinkwater, Moore, & Bird., 2012, p. 890).
Squat variations:
Most people put squatting in the 'too hard basket, which might be the case if you want to do a pistol squat, Olympic squat or squat to the ground. Don't forget that squatting takes on many forms and the most important thing to consider is the level of function your patient has and where the squat should start.
Here are a few ideas.


For those who can't do a free standing body weight squat
Assisted squat using a rail to provide balance.
Sit to stand from a chair or lower/higher bench height.
Fit ball squat.
Free standing squat - partial, parallel or full depth.
Wall squat - foot position short or long, or split.
Single leg squat
Pistol squat.
Olympic squat.
Jump squats.
Front squat and back squat.
And then consider bars, free weights, kettle bells, medicine balls, wobble board, bosu ball and other pieces of equipment that will challenge to difficulty, complexity and stability of the squat.


Take home message
For the best squatting technique:
- When squatting aim to keep the hip, thigh and knee movement equal and at the same time. Also aim to keep the trunk and shin bone at a similar angle to each other.
- As squat depth increases, gluteus maximus activity increases.
- Hip and knee extensor muscles work harder with a wider stance.
- Foot rotation doesn't play a large role in the exercise demands of a squat and is used to improve patient comfort.
- For lower PFJ compressive forces work between 0-50 degrees flexion and consider progressing from a wall squat to single leg squat to increase the work load.
- For power and speed use loaded partial to parallel squats and for work load use full squats.
- For a patient to be able to perform a full squat with flat heels they require ~95 degrees hip flexion and ~40 degrees ankle dorsiflexion (Schoenfeld, 2010).
My personal preference is to start with an assistance squat or a sit to stand. This allows patients to gain an understanding of the movement pattern required to achieve a parallel squat position. From there they can practise the concentric phase of squatting with or without weights. Once this is achieved my patients are taught to tap the bench rather than completely rest and overtime the bench is removed and a parallel squat can be performed without assistance. After that the harder progressions are a matter of correct technique, conditioning and practise.
Sian
References
Almosnino, S., Kingston, D., & Graham, R. B. (2013). Three-Dimensional Knee Joint Moments During Performance of the Bodyweight Squat: Effects of Stance Width and Foot Rotation. Journal of applied biomechanics, 29, 33-43.
CATERISANO, A., MOSS, R. E., PELLINGER, T. K., WOODRUFF, K., LEWIS, V. C., BOOTH, W., & KHADRA, T. (2002). The effect of back squat depth on the EMG activity of 4 superficial hip and thigh muscles. The Journal of Strength & Conditioning Research, 16(3), 428-432.
Drinkwater, E. J., Moore, N. R., & Bird, S. P. (2012). Effects of changing from full range of motion to partial range of motion on squat kinetics. The Journal of Strength & Conditioning Research, 26(4), 890-896.
Escamilla, R. F., Fleisig, G. S., Lowry, T. M., Barrentine, S. W., & Andrews, J. R. (2001). A three-dimensional biomechanical analysis of the squat during varying stance widths. Medicine and science in sports and exercise, 33(6), 984-998.
Escamilla, R. F., Fleisig, G. S., Zheng, N. A. I. Q. U. A. N., Lander, J. E., Barrentine, S. W., Andrews, J. R., ... & Moorman, C. T. (2001). Effects of technique variations on knee biomechanics during the squat and leg press.Medicine and science in sports and exercise, 33(9), 1552-1566.
Escamilla, R., Zheng, N., Macleod, T., Brent Edwards, W., Imamura, R., Hreljac, A., ... & Andrews, J. (2009). Patellofemoral joint force and stress during the wall squat and one-leg squat. Medicine+ Science in Sports+ Exercise, 41(4), 879.
Gullett, J. C., Tillman, M. D., Gutierrez, G. M., & Chow, J. W. (2009). A biomechanical comparison of back and front squats in healthy trained individuals. The Journal of Strength & Conditioning Research, 23(1), 284-292.
Paoli, A., Marcolin, G., & Petrone, N. (2009). The effect of stance width on the electromyographical activity of eight superficial thigh muscles during back squat with different bar loads. The Journal of Strength & Conditioning Research, 23(1), 246-250.
Schoenfeld, B. J. (2010). Squatting kinematics and kinetics and their application to exercise performance. The Journal of Strength & Conditioning Research, 24(12), 3497-3506.